


Introduction
Clinical depression is anything but a ‘usual suspect’ in public opinion research. It has not been on the radar of those modelling referendum choice. In this article, we suggest that it should be. One simple reason is its prevalence. Survey evidence suggests that one in six English adults suffer from a common mental disorder such as depression or anxiety, and more than one third of those seek mental health treatment (McManus et al. Reference McManus, Bebbington, Jenkins and Brugha2016). Depression was set to become the second costliest disease to society by this year (Lecrubier Reference Lecrubier2001) and is defined by the WHO as a leading cause of disability worldwide. But the core of this article is the second reason: that depression is a major influence over those cognitive and affective processes that are at the heart of referendum choice – particularly when, as often, that choice is between the status quo and change. On one hand, one facet of depression is the kind of dissatisfaction with life that is associated with voting for change. On the other hand, cognitive models of depression portray sufferers as less inclined to seek information about change, more pessimistic about its benefits and more likely to exaggerate its potential costs. This leads to our central hypothesis: that depressivesFootnote 1 are disproportionately likely to support the status quo option in referendums.
In this article, we explore this territory and test that hypothesis in the case of the ‘Brexit’ referendum in the UK. Using data from the Understanding Society panel survey, we find evidence of a depression effect on pre‐referendum preferences. Those diagnosed with clinical depression were appreciably more likely to favour the status quo of remaining in the European Union (EU). Our claim that this contrast is driven by different orientations to change wins support from an interesting further finding. Once the referendum result had sunk in and the psychological status quo had therefore changed, depressed individuals moved strongly towards Leave.
Our findings extend two strands of research. The first is the growing evidence of health effects on mass politics (Carpenter Reference Carpenter2012). So far, much of this has focused on behaviour. We know, for example, that turnout is lower among voters with poor physical health (Schur et al. Reference Schur, Shields, Kruse and Schriner2002; Mattila et al. Reference Mattila, Söderlund, Wass and Rapeli2013; Pacheco & Fletcher Reference Pacheco and Fletcher2015) or poor mental health – including depression (Ojeda Reference Ojeda2015; Sund et al. Reference Sund, Lahtinen, Wass, Mattila and Martikainen2017; Burden et al. Reference Burden, Fletcher, Herd, Moynihan and Jones2017; Couture & Breux Reference Couture and Breux2017; Ojeda & Pacheco Reference Ojeda and Pacheco2019; Ojeda & Slaughter Reference Ojeda and Slaughter2019). Yet to date we know very little about the impact of psychological health on political attitudes. The second concerns risk orientations and their impact on attitudes and voting. This began by noting risk‐averse voters’ reluctance to support challengers over incumbents (Kam & Simas Reference Kam and Simas2012; Eckles et al. Reference Eckles, Kam, Maestas and Schaffner2014). Further studies, applying the same logic, have revealed a similar reluctance among these voters to support change in referendums – including, most recently, voting for Brexit (Steenbergen & Siczek Reference Steenbergen and Siczek2017). Our argument is that one component of depression, especially in its more severe form, is a heightened or clinical form of such risk‐aversion – with predictable consequences for voting behaviour.
In what follows, we first examine the impact of depression on cognitive processing in general and then referendums in particular. Then we introduce the Brexit case and our data before reporting and discussing our findings. While data constraints mean that we cannot test the risk mechanism directly in this article, we find clear evidence of the hypothesised tendency: those with depression are disproportionately supportive of the status quo.
Decision‐making in depression
Depression affects decision‐making. It is associated with abnormalities in decision‐related areas of the brain (Palazidou Reference Palazidou2012), and cognitive psychologists have shown that depression shapes multiple domains such as memory, attention, perception and interpretation (for a review, see Gotlib & Joormann Reference Gotlib and Joormann2010). Our central argument here is that all of this will leave depressives particularly attached to status quo options. It has three main strands, concerning, respectively, quantity, interpretation and weighting of information about change. First, the low motivation, low energy and indecisiveness that feature in depression mean that sufferers are less willing to research and assess change. The resulting lack of information widens the uncertainty around their estimates of the benefits of voting for change. Second, the central tendency of those estimates is biased downwards. Depression is associated with a persistent underestimate of expected benefits arising from biases in priors and in the selection of information. Third, even if this skewed calculation still leaves the benefits of change exceeding the costs, the latter will weigh more heavily in depression sufferers’ decision‐making. In this section, we briefly expand on these arguments, drawing on both seminal and more recent empirical work on depression.
According to Beck's seminal cognitive approach (Beck Reference Beck1967; Beck et al. Reference Beck, Rush, Shaw and Emery1979), which still underpins many computational models today, individuals vulnerable to depression develop self‐schemas – organised structures that facilitate the way in which humans process information – considered maladaptive or dysfunctional because the encoding and retrieval of information is negatively biased. When depressive self‐schemas are activated by negative life experiences, cognitive errors and negative automatic thoughts ensue. These thoughts usually take the form of a negative view of oneself, the world and the future (i.e., the negative triad).
Depressed people mistrust positive emotions (Paulus & Yu Reference Paulus and Yu2012). They give greater weight – and have readier access in working memory – to negative considerations and are prone to rumination on them (Nolen‐Hoeksema Reference Nolen‐Hoeksema2000; Gotlib & Joormann Reference Gotlib and Joormann2010; Robinson & Roiser Reference Robinson, Roiser, Robbins and Sahakian2016). Moreover, many studies (reviewed by Dozois & Beck Reference Dozois, Beck, Dobson and Dozois2008) highlight the tendency among depressed individuals to filter information and respond to stimuli in a way that confirms their pessimistic assumptions. They are more negative in their recall of feedback, make more negative self‐evaluations, more internal attributions for failure, and are more downbeat about the consequences of action (e.g., Coyne & Gotlib Reference Coyne and Gotlib1983).
Pessimism is thus key to decision‐making in depression. Bayesian decision‐theoretic approaches from computational neuroscience (Huys et al. Reference Huys, Daw and Dayan2015) suggest that depression is related to under‐researching and under‐estimating the benefits of change due to biases in priors. Two core factors in the cognitive model of depression are helplessness, the belief that future outcomes are uncontrollable, and anhedonia, the inability to experience and derive pleasure from rewards (Abramson et al. Reference Abramson, Seligman and Teasdale1978; Elliott et al. Reference Elliott, Sahakian, McKay, Herrod, Robbins and Paykel1996). Both can be formalized as priors directly influencing those two facets of pessimism – under‐researching and under‐estimating the benefits of change – mentioned above. On helplessness, depressives tend to attribute negative outcomes to internal, global and stable factors and to attribute positive outcomes to external, specific and unstable causes. The former is a particularly stubborn feature of what Seligman et al. (Reference Seligman, Abramson, Semmel and von Baeyer1979) call depressives’ attributional style. If the world is believed not to be controllable, negative outcomes are assigned to change, hence reducing the value of unknown options and preventing their exploitation (Huys et al. Reference Huys, Daw and Dayan2015: 14). When it comes to anhedonia, if depression is associated with low expected average reward then this ‘will reduce the tendency to act and thereby the rate at which information from the environment is gleaned’ (Huys et al. Reference Huys, Daw and Dayan2015: 13–14). Depressives are thus prone to carry on doing a limited set of actions even if there are more profitable alternatives, showing less sensitivity to reward but more to punishment (Smoski et al. 2008; Cella et al. Reference Smoski, Lynch, Rosenthal, Cheavens, Chapman and Krishnan2010).
The consequences are spelled out in Leahy's (Reference Leahy1997) portfolio theory, an account of decision‐making in depression based on models of financial investment. Depressives ‘are pessimistic about outcomes, suffer losses more than they enjoy gains, believe they have few current or future resources, are less likely to generalize positives and are more likely to generalize negatives’ (Leahy et al. Reference Leahy, Tirch and Melwani2012: 363). This translates into strongly risk‐averse attitudes and behaviour. In the lab, studies of animal models of depression (Shabel et al. Reference Shabel, Murphy and Malinow2014) have shown that rats with congenitally learned helplessness are more risk‐averse than wild‐type control rats. The same is true of humans performing cognitive tasks, with depressive individuals selecting fewer advantageous cards (Han et al. Reference Han, Klimes‐Dougan, Jepsen, Ballard, Nelson, Houri and Cullen2012), less risky card decks (Smoski et al. Reference Smoski, Lynch, Rosenthal, Cheavens, Chapman and Krishnan2008) and less shifting of strategies (Cella et al. Reference Cella, Dymond and Cooper2010). The hallmark of depression is ‘a strategy to avoid further loss, resulting in active attempts to resist change as evidenced in motivated negative cognition (e.g., trying to prove it is hopeless)’ (Leahy et al. Reference Leahy, Tirch and Melwani2012: 363). The link with status quo bias is very clear.
Depression and the Brexit referendum
Depression, risk and status quo bias
All votes represent to some extent a choice between the status quo and change. In elections, this comes in the form of incumbents (whether parties or candidates) versus challengers. In referendums, the contest between status quo and change is usually even more clear‐cut. When those voters went to the polls on 23 June 2016 to answer the question ‘Should the United Kingdom remain a member of the European Union or leave the European Union?’, the verbs confirm that this was another referendum open to a status quo versus change framing (even if, as discussed below, the political reality was not as clear‐cut as that). As emphasised by de Vries (Reference De Vries2018), the basic structure of decision is straightforward: a comparison of satisfaction with current arrangements and estimated satisfaction under the new arrangements. The more significant the proposed change, the more limited the available information and hence the greater the uncertainty around that estimate.
In the light of this, it is not surprising that research has linked risk attitudes to referendum voting – often making the same arguments that underlie our specific hypothesis about depression. Several studies have adduced a tendency to risk aversion – the ‘better the devil you know’ mindset – within broader electorates to explain a late swing towards status quo options in direct democracy (LeDuc Reference LeDuc2003; see also Bowler & Donovan Reference Bowler and Donovan1998; Christin et al. Reference Christin, Hug and Sciarini2002). And there is emerging individual‐level evidence that more generally risk‐averse citizens tend towards the status quo option in referendums (Verge et al. Reference Verge, Guinjoan and Rodon2015; Morisi Reference Morisi2016). Two examples are particularly relevant here. The first is an analysis by Nadeau et al. (Reference Nadeau, Martin and Blais1999) of voting in Quebec's 1995 independence referendum. They find that, while risk‐accepting voters tended to weigh up expected costs and benefits fairly neutrally, the most risk‐averse instead gave heavy weight to the possibility that independence would prove disastrous. This is very reminiscent of the psychological processes described earlier. The second is Steenbergen and Siczek's (Reference Steenbergen and Siczek2017) evidence from the Brexit referendum itself. They found the odds of voting for Brexit to have been 105% greater among the most risk‐willing compared to the most risk‐averse.
Arguably, that effect would have been stronger had the status quo versus change distinction not been a little blurred in this (as probably in any) referendum campaign. For one thing, voters politically socialised before 1973 could remember when the UK was not a member of the European Union (in its earlier incarnation as the European Economic Community). In other words, for a large chunk of the electorate, leaving the EU could be seen as a return to the status quo ante rather than as a shift to something new. This set a limit on the perceived uncertainty posed by Brexit. Another argument is that a Remain vote would not entrench the status quo given that the institutions of the EU are evolving, and so in turn is the meaning of membership (de Vries Reference De Vries2018: 43). Given the UK's highly qualified version of EU membership and the lack of mainstream political support for changing that, it seemed unlikely in 2016 that a Remain vote would trigger further integration in a hurry. But the Leave campaign raised more specific prospects, a vivid example being the possibility of Turkish membership and its implications for immigration. With a clear majority of people (i.e., not just Leave voters) regarding Turkish accession within 10 years as likely (WhatUKThinks 2016a), this pointed to significant change via the status quo option.
The extent to which Remain versus Leave was seen by voters as status quo versus change is ultimately an empirical question. While no polling data address it head on, we can at least approach it via an eve‐of‐referendum YouGov poll that asked respondents to designate each option on a scale from ‘very risky’ to ‘very safe’. Responses by that point had become highly partisan and so Table 1 shows the results not just for all respondents but also for the subset still undecided at that late stage. The pattern is clear regardless. Insofar as those suffering from depression react differently to potentially risky changes, there is reason to expect such a difference to have manifested itself in the case of Brexit. This chimes with those risk‐aversion effects already cited from Steenbergen and Siczek (Reference Steenbergen and Siczek2017).
Table 1. Perceived riskiness of Leave and Remain options on referendum

Source: WhatUKThinks (2016b).
As illustrated by the example of immigration from Turkey, the fact that a Remain vote was widely seen as carrying at least some risk is owed in part to the success of the Leave campaign. This highlights an important feature of this referendum, namely that both sides made attempts to stoke voters’ fears about the alternative (Galpin Reference Galpin2016). If it were the case that only the Remain side had fought a negative campaign, seeking to catastrophise the economic risks of Brexit, then a disproportionate Remain vote among depression sufferers would be more ambiguous: it might reflect status quo bias but it might instead be just a specific response to that campaign. It is therefore significant that the Leave side had its own ‘Project Fear’,Footnote 2 emphasising to voters – including depression sufferers – the risks, especially about the extent and impact of immigration, of remaining in the EU. We are not arguing that Leave relied exclusively or even mainly on negative or fear‐driven campaigning – there were also strong positive messages about parliamentary and financial sovereignty. Our point is simply that both Remain and Leave campaigns sought to touch nerves that are particularly exposed or sensitive among those with clinical depression.Footnote 3 Hence, if depressives were particularly inclined towards the status quo, this has to do with the structure of the choice as well as the campaign tactics deployed.
Depression, dissatisfaction and voting for change
We need to recognise two powerful challenges to our hypothesis that depression will predict support for the status quo. First, evidence from electoral research shows that dissatisfaction or disillusionment drives support for change (e.g., Franklin et al. Reference Franklin, Marsh and McLaren1994; Hooghe et al. Reference Hooghe, Marien and Pauwels2011) – a pattern again visible in the EU referendum when those distrustful of politicians and disapproving of government performance voted disproportionately for Brexit (Hobolt Reference Hobolt2016). And dissatisfaction need not be specifically political in order to prove electorally relevant. Subjective well‐being (or ‘happiness’, for short) boosts support for the status quo (Flavin & Pacek Reference Flavin and Pacek2014) and for incumbent parties (Liberini et al. Reference Liberini, Redoano and Proto2017a) – even if that happiness is driven by recent success for the local college football team (Healy et al. Reference Healy, Malhotra and Mo2010) – and was strongly associated with support for the major shake‐up to the political status quo that was the election of Donald Trump (Sides & Tesler Reference Sides and Tesler2016). Most importantly for present purposes, Liberini et al. (Reference Liberini, Oswald, Proto and Redoano2017b) show that those reporting themselves most dissatisfied with life were significantly more likely to support Brexit in 2016, even controlling for various other life circumstances.
There is obvious conceptual and empirical overlap between dissatisfaction and depression. On one reading, the two are distinct (albeit quite highly correlated) dimensions of mental health (Headey et al. Reference Headey, Kelley and Wearing1993). A different view is that dissatisfaction, often referred to in this context as ‘low mood’, should be regarded as one of the components of depressive disorder – as in the standard diagnostic tests for depression (Gruenberg et al. Reference Gruenberg, Goldstein, Pincus, Licinio and Wong2005). Crucially, this is a different component from the cognitive biases that drove our arguments about fear of change. Horwitz et al. (Reference Horwitz, Wakefield, Lorenzo‐Luaces, DeRubeis and Strunk2016) set out how mood and cognition have long been separated in understanding and measurement of the disorder, referring to a ‘traditional distinction between melancholic and neurotic depression’ (p. 22). For present purposes, that distinction can be reframed as between dissatisfaction and the cognitive pessimism or hopelessness outlined above.
Where does this leave our central hypothesis? First, since dissatisfaction and cognitive pessimism point in opposite directions when it comes to referendum voting, we can regard depression sufferers as cross‐pressured. Second, we suggest that the balance of those competing pressures changes with the severity of depression. Dissatisfaction might be the most prominent symptom of mild depression but, in more severe or clinical cases, it is likely to be overridden by the cognitive dynamics we set out above. This does not imply that the clinically depressed would be satisfied with the status quo. The point is simply that they are prone to see change as likely – or, at least, too likely– to be even worse. We therefore still anticipate that depression will predict voting for the status quo while dissatisfaction predicts voting for change. Third, since depression and dissatisfaction are likely to be quite strongly correlated, a clean test of those expectations requires us to estimate the effect of each variable while controlling for the other. Otherwise, the omitted variable would operate as a suppressor.
The second challenge to that central hypothesis comes via the notion of ‘locus of control’. As argued above, one recurring cognitive symptom of depression is external locus of control: a sense that one is at the mercy of – even overwhelmed by – the outside world. This creates a wish to regain control and, according to some recent work on mental health and political participation, this can translate into more active engagement to achieve change – at least in less demanding activities such as signing a petition or boycotting a product (Söderlund & Rapeli Reference Söderlund and Rapeli2015; Couture & Breux Reference Couture and Breux2017). In particular, Söderlund and Rapeli (Reference Söderlund and Rapeli2015) argue that depressives’ customary reluctance to participate can be overcome by that same external locus of control. If those with depression blame their personal status quo on current policy and politicians, this could translate into support for change – including in a referendum. That might be particularly the case where, as with sovereignty referendums in general and the Brexit referendum in particular, the change option is framed as an opportunity to regain control. The slogan ‘take back control’ was at the heart of Leave's campaigning (Evans & Menon Reference Evans and Menon2017: 88; Hobolt Reference Hobolt2016: 1262).
However, again there is a caveat given the way in which depressives assess new or ‘change’ options. Their feeling that the world is not controllable is one that is learned early and deeply instilled (e.g., see Abramson et al. Reference Abramson, Seligman and Teasdale1978). While potentially attracted by the notion of regaining control, they are also liable to be sceptical about the prospect. A feeling of hopelessness or helplessness may attach to change options just as much as to the status quo. Overall, then, while acknowledging that a regaining‐control message is likely to appeal to depression sufferers, we maintain that the tendency asserted in our central hypothesis – about resistance to change among depressive voters – will predominate.
Depression and adjusting to change
One final point about depression and the Brexit case is worth noting, particularly given that our data source offers responses after as well as before the referendum. If depression sufferers feel rather at the mercy of political events rather than in control of them, then it may be that their attitudes are similarly compliant with context – including the kind of change in context brought about by the result of the Brexit referendum. While those with strong opinions on the issue will stick to their position even after defeat, those – notably sufferers from depression – whose main priority is just to avoid political upheaval might well be inclined to move towards the new status quo heralded by the result. The major premise here is that depressives are attracted to options that, in simple terms, ‘make an issue go away’. The minor premise is that, once the votes were cast and the new Prime Minister had announced that ‘Brexit means Brexit’, leaving the EU had become that option. Post‐referendum polls identified a split among Remain voters: roughly half wanted the result ignored or overturned in another referendum; the other half just wanted politicians to get on with enacting the result (e.g., YouGov 2017). Our argument is that depression sufferers, for whom notions like ‘overturning’ are particularly unappealing, are likely to be over‐represented in the second group.
Consistent with our focus throughout this article, the status quo we refer to here is more psychological than institutional. What would matter is not so much whether the change proposed in the referendum had taken place but whether voters, and depression sufferers, had come to believe and accept that it was going to do so. This might be a long process. Whereas a change of government hands incumbency advantage straight over, a referendum vote for change takes a while to shift the status quo in voters’ minds. The picture is further blurred by the rhetorical battle over the terms of departure. Many Remain campaigners promptly began arguing for a deal having so much in common with continuing membership that Brexit would be palatable to all but the most risk‐averse. Yet parallel talk of ‘cliff edges’ (e.g., Campbell Reference Campbell2016) will have had exactly the opposite effect on depressive voters already worried at the prospect of leaving the EU. Overall, then, we are not arguing that the vote on 23 June cleanly and swiftly installed leaving the EU as the new status quo. Nevertheless, our central point holds. If at least part of depression sufferers’ pre‐referendum opposition to change was driven by attachment to the status quo rather than to the EU, then that source of opposition will dissipate as the context changes.
Data and measures
Our data source is Understanding Society, a household panel study running under that name since 2009. Wave 8 of the panel went into the field at the beginning of 2016 and, in view of the impending referendum, the designers added a question about support for EU membership onto that wave. We were among those research teams allowed early access to Wave 8 data, with interviews between 5 January 2016 and 6 April 2017 (although most, 92%, come from the referendum year of 2016).Footnote 4 This gives us responses from both before and after the referendum on 23 June – enabling us to check whether it brought about any change in the relationship between depression and support for Brexit.
The first wave of Understanding Society began with a probability sample.Footnote 5 We apply the survey's standard weights to adjust for non‐random attrition in later waves (and to adjust for various design features – see Section S1 of the Online Appendix). A side‐effect of this weighting is to reduce the Wave 8 sample size (from 21,076 to 13,188) and hence statistical power. When we eliminate those either missing on our clinical depression measure or who did not report an opinion on EU membership, this drops to 12,020 – still large in absolute terms.
The dependent variable question was worded as follows: “Should the United Kingdom remain a member of the European Union [coded 0] or leave the European Union [coded 1]?” For the survey designers, this had advantages over a referendum vote question: the wording would not need changing after 23 June, and it could be asked of all respondents rather than only those eligible to vote. Unfortunately, by asking about attitudes rather than voting behaviour, this question precludes a test of the association between depression and turnout. Another limitation here is that the question will have taken on an additional dimension once the result was in, asking Remain voters to set their ongoing preferences for EU membership against any perceived imperative to enact the referendum verdict. The upshot for our purposes is that support for Brexit is likely to have taken a step change upwards following 23 June, so any change we observe in the responses of the depressed has to be set against that across‐the‐board shift. In practice, however, that overall shift turns out to be small. Taking the sample as a whole, the percentage support for leaving the EU was 41.5% among pre‐referendum and 46.1% among post‐referendum respondents. This reinforces the idea that the measure continued to tap attitudes on the issue more than the implementation of the referendum results.
Our primary independent variable is a dummy, diagnosed depression. Respondents are asked ‘Has a doctor or other health professional ever told you that you have any of the conditions listed on this card?’, and ‘Clinical Depression’ is among the items listed. If they choose that item, they are then asked ‘Do you still have clinical depression?’ In addition, respondents are also asked ‘Since ff_IntDate has a doctor or other health professional newly diagnosed you as having any of the following conditions? If so, which ones?’ Respondents answering ‘yes’ to one of those questions in Wave 8 – that is, long‐term panellists or new joiners reporting depression – were coded as 1 on our dummy measure. In Wave 1, this amounted to 5% of the sample. Everything we know about depression implies disproportionate attrition among this group, but it is nonetheless startling that, by Wave 8, so many of these respondents had dropped out of the panel such that only 1% of the sample was now coded as diagnosed. It is highly unlikely that those remaining depression sufferers are an unbiased sample of the initial group. If depression draws people away from the panel, then those remaining are likely to be less acute cases. The same is true when we consider the fact that those suffering from severe depression are less likely to take part in this kind of relatively demanding survey in the first place (Korkeila et al. Reference Korkeila, Suominen, Ahvenainen, Ojanlatva, Rautava, Helenius and Koskenvuo2001; Volken Reference Volken2013). All of this makes our analyses a conservative test of the difference between (all) clinical depressives and the rest of the population. Further conservatism is enforced by the fact that, since 1% of even our very large sample is a rather small number of clinically depressed people (weighted N = 104), our tests are not highly powered.
Our other main independent variable, life dissatisfaction, is a standard seven‐point life satisfaction scale (reverse‐scored and rescaled from 0 to 1). As expected, it is strongly positively associated with diagnosed depression: the polychoric correlation (offering more traction with binary variables than Pearson's r) between the two is 0.40. This underlines the need to control for dissatisfaction when seeking the effect of depression (and vice versa).
In the regressions, we also control for a list of other variables that have been shown to predict Brexit referendum voting (Hobolt Reference Hobolt2016) and may also correlate with depression: age, age squared, sex, general health, marital status, social class, respondents’ expectations about their household's financial future, party identification, highest educational qualification and income. Summary statistics are reported in Table S3 in the Online Appendix. Due to widespread missing values in the latter three socio‐demographic variables, we present two versions of the main model – one with and one without them (the latter reflecting the need to conserve observations given how few depression sufferers are in the sample).
These data allow us to control for the key players rather than providing a thoroughly specified model of referendum voting. The latter job has been well done elsewhere (e.g., Hobolt Reference Hobolt2016; Clarke et al. Reference Clarke, Goodwin and Whiteley2017). Our aim is to provide the best test of the non‐spurious association between depression and Brexit preferences. And there are grounds for confidence here. First, as a clinical and indeed partly chemical condition, depression is harder to predict with sociological or economic models than would be, say, life dissatisfaction.Footnote 6 The chances that we have failed to control for a powerful socio‐demographic predictor of both clinical depression and Brexit voting are remote. Second, depression comes close to the mouth of what electoral researchers call the ‘funnel of causality’ (Campbell et al. Reference Campbell, Converse, Miller and Stokes1960). Even variables like education level are unlikely to be wholly prior to depression, while many customary controls in models like this, such as party identification, are likely to be wholly posterior. If the latter are omitted, we miss an opportunity to elucidate the mechanisms by which depression influences Brexit attitudes, but we do not misestimate its total causal effect.
The biggest such missed opportunity concerns risk orientations, which are sadly not available in Wave 8 nor the immediately preceding waves of Understanding Society. This limits our capacity to test directly the mechanism driving the central hypothesis. However, data from Wave 1 (in which, unlike the referendum wave, both questions were asked) confirm that depressive respondents scored on average more than one point (around half a standard deviation) lower on a 0–10 risk‐acceptance scale. So the first step in that mediation chain is confirmed. Moreover, the availability of data from before and after the referendum provides a useful if indirect indicator. If what distinguishes depression sufferers is the way that they deal with risk and uncertainty, then we would expect their opinions to be more distinct before the referendum than once the results and its implications have filtered through.
Results
We begin with simple crosstabulations between our dependent and main independent variables. Table 2 therefore simply reports the percentage support for leaving the EU among those who are and those who are not diagnosed with depression, along with Fisher's exact tests for significance. We first show the results for the whole data collection period and then break these down by timing of interview with respect to polling day. Across the sample as a whole (i.e., pre‐ and post‐referendum responses), support for Leave was 35.7% among the clinically depressed compared to 44.3% among the non‐depressed. This is in the hypothesised direction, but even a gap of nearly nine points is not quite statistically significant given the small number of clinically depressed respondents. However, in the right‐hand panel, a more striking pattern emerges which is not only consistent with our hypotheses but meets significance criteria despite those small numbers. Prior to the referendum, depressed voters were as many as 19 percentage points more likely to support Remain, a difference significant at the p < 0.01 level. Among post‐referendum respondents, that gap closes entirely. Both groups swing somewhat to Leave, understandably now that this position had gained legitimacy from the outcome. But the swing is far larger among depression sufferers. These results provide encouragement for proceeding with the multivariate analysis.
Table 2. Crosstabulations of depression and support for Leaving the EU
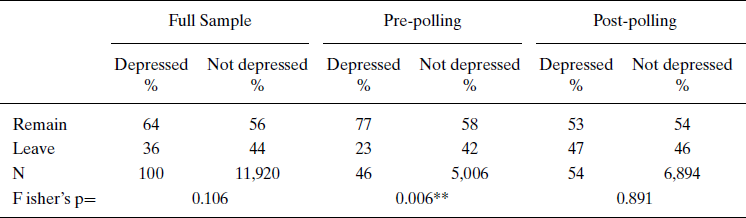
Table 3 reports three logistic regression models predicting support for leaving the EU, each of which includes depression and life satisfaction as well as general health and the core socio‐demographic variables mentioned above. To accompany each coefficient for depression, we calculate predicted probabilities for the depressed and non‐depressed based on that model and use these to report an implied percentage point difference in support for Brexit.
Table 3. Logistic regression models predicting support for Leaving the EU

*p ≤0 .05;
**p ≤ 0.01; two‐tailed tests; standard errors in parentheses.
Model 1 is based on the full sample: that is, responses from both before and after the referendum. The first thing to say is that the bivariate effect just described is robust against these controls. The effect of clinical depression is negative as expected and, while not statistically significant, remains quite substantial in size. The gap in predicted probabilities of Leave support between clinically depressed and other respondents is estimated at almost 10 percentage points. Meanwhile, the effect of life dissatisfaction is also non‐significant. Since this will not be an issue of statistical power, it probably has more to do with the model including detailed controls for many of the reasons why respondents might be dissatisfied with life: poor health, straitened economic circumstances, marriage break‐up, and so on. There are at least indications, however, of the contrast hypothesised earlier: that dissatisfaction with life would prompt support for change while the specific cognitive dynamics of diagnosed depression led to support for Remain.
We argued earlier that, if indeed depressives were registering support for the status quo rather than for the EU per se, then that support should ebb once the referendum result indicated a shift in the status quo. The purpose of Models 2 and 3 is to test this pre‐post contrast more formally, analysing the full sample but including an interaction between depression and the timing of interview. This also allows for a slightly more refined measure of timing (even if it remains somewhat crude given the limited number of cases for analysis). Our Time variable has four categories and is coded as 1 for interviews more than three months before the referendum date, 2 for the final three months of the campaign, 3 for the three months after the referendum, and 4 for more than three months after the referendum date. This allows for the possibility that depression sufferers adjust rather more slowly to the change heralded by the Brexit vote. That possibility is clearly borne out by the results from Model 2 and the pattern illustrated in Figure 1, which plots predicted probabilities of supporting Brexit among those with clinical depression and the rest of the sample. Up to and in the immediate aftermath of the referendum, depressives remained clearly and statistically significantly less likely to support change. Yet it seems that, once they had digested the referendum result and adjusted to the notion that this change was coming anyway, if anything they were more likely to support Brexit and less likely to favour the now disruptive option of remaining in the EU.

Figure 1. Effects over time of clinical depression on the probability of supporting Brexit. [Color figure can be viewed at wileyonlinelibrary.com]
The main point from Model 3 is to confirm that this pattern is robust to controlling for the full range of background variables – now including party identification, education and income which were omitted from Models 1 and 2 (due to the preponderance of missing values). While the results from the control variables are not central to our purposes, it is worth noting that they confirm the consistent patterns from previous work (Hobolt Reference Hobolt2016; Clarke et al. Reference Clarke, Goodwin and Whiteley2017; Alabrese et al. Reference Alabrese, Becker, Fetzer and Novy2019). Leave was a more popular option among older people, men, those with lower education and those on lower incomes. It was naturally more popular among identifiers with the Eurosceptic UK Independence Party but less popular among those identifying with Remain‐supporting parties, Labour and the Liberal Democrats.
One less predictable result is that the effect of general health runs in the opposite direction to that of depression. This tends to undermine one alternative explanation for our depression effect: that sufferers were oriented towards Remain because they were particularly sensitive to the risks that leaving the EU posed to the UK healthcare system (Esmaeilzadeh & Mirzaei Reference Esmaeilzadeh and Mirzaei2018). If anything, those most in need of that system were more likely to support Leave. Perhaps they were persuaded by the infamous bus and its promise of extra NHS funding in the event of Brexit (Reid Reference Reid2019). More likely, poor physical health contributed to that broader feeling of unhappiness with the status quo which Liberini and colleagues (Reference Liberini, Oswald, Proto and Redoano2017b) found to drive support for Leave.
Conclusions
In this article, we find support for an innovative hypothesis: that those diagnosed with clinical depression are significantly more likely to favour the status quo in the run‐up to referendums. There has been very little research into the attitudinal implications of depression in a political context.Footnote 7 At the same time, our findings are deeply rooted in some long‐established findings about the ways in which depression shapes the acquisition and processing of information and the resulting decisions. The pattern of results here, with depressed individuals being markedly more likely to support remaining in the EU in the run‐up to polling day but not for long thereafter, is consistent with our argument that their reactions owed less to the substance of the issue and more to opposing the uncertainty and disruption of change. It makes sense that, once depression sufferers were persuaded that ‘Brexit means Brexit’, they were then disinclined to support a Remain option that had in some ways become the disruptive change.
The preceding paragraph involves speculation about psychological processes that goes some way beyond the data here. To some extent, this is inevitable in public opinion research but it is also a particular consequence of using Understanding Society. It is a household panel survey, not a psephological instrument, and hence lacks useful ‘mechanism’ questions asking about, for example, the perceived risks of Brexit. (There are of course alternative surveys allowing much more complete modelling of voting in the EU referendum – and another obvious instance, the Scottish independence referendum in 2014 – but these lack the depression measures even more central to our purposes. The same is true of national election surveys, frustrating the aim of extending this research to another obvious instance of status quo bias: voting for incumbents over challengers.)
Causal inference here, then, hinges on the striking difference between the pre‐ and post‐referendum associations between depression and support for leaving the EU. Our contention is that this reflects Leave becoming, by the end of 2016, the option seen by many depressives as reflecting less upheaval – in the phrase used earlier, the option that would ‘make the issue go away’. Of course, there will be individual differences as within the electorate as a whole: some will have continued to fear the change of leaving the EU, while others had strong views on the issue that were unconnected to their depression. Nonetheless, that striking and significant shift in opinion is consistent with our argument about support for a shifting status quo. And it is hard to think of alternative explanations for the pattern in Figure 1. The much greater willingness among depressives to support Brexit post‐referendum might at first glance be attributed to a legitimacy effect, but then there is little such shift among non‐depressives and we have no reason to expect depressives to give disproportionate weight to legitimacy concerns. A psychological variant of this argument is one in which depressives seek the security of being in the majority. Since a Remain vote was widely heralded before the referendum, someone determined to ‘follow the crowd’ would then move across the fence to Leave once the result was in. However, studies of depression provide little theoretical or empirical basis for such conformity. Our suggested mechanism, dislike of change, finds much more support. One other point about the pre‐post shift in opinion here is that it runs against the grain of another possible impact of the referendum: a dent in the mental health of those who were on the losing side. It is far beyond the scope of this article to assess the extent of ‘Brexit anxiety’ (Hughes Reference Hughes2019) or depression among Remain supporters. Here, the key point is that this would imply a post‐referendum tightening of the link between depression and Remain support. In fact, we see a loosening.
These findings about depression are based on a measure of diagnosis rather than symptoms. While there are advantages in the relative objectivity of a diagnosis‐based measure, there are obvious limitations, too. Many depressed people have not sought diagnosis, and the propensity to do so has often less to do with severity of symptoms than with resources and access to the healthcare system. Moreover, given the stigma of mental illness, there may be a stronger social desirability bias against admitting a clinical diagnosis than reporting various symptoms. It would obviously have been preferable to be able to include more detailed measures of the kind of anxiety symptoms and cognitive biases driving our main hypothesis. Yet such measures are hard to obtain via self‐reports in a population survey. More common are measures of symptoms like low mood or inhibited social functioning. While important components of depressive disorder, these have more in common with the general dissatisfaction that drives support for change than they do with the dynamics that we contend drove support for the status quo.Footnote 8 As such, they are not ideal for testing our hypothesis or its underlying mechanisms.
It is hard to estimate precisely the incidence of major depressive disorder. The diagnosis and medication of clinical depression is growing, but this may say more about the easing of stigma and a growing willingness to diagnose and treat depression. What is clear, and should not be obscured by the small sample available for our analysis, is that depression is not a rare condition. A substantial proportion of people experience the patterns of thinking whose political consequences are explored in this article. If that proportion is growing, then the likely impact on risky choice – and on the potential of campaigns playing on those risks and fears – is growing too. This reinforces the normative ramifications of our findings. A central tenet of the social model of disability (e.g., Oliver Reference Oliver2013) was that a health impairment of any kind constitutes a disability only when adverse features in the context make it so. And an inclusive democracy requires that public debate as well as political participation are accessible for all citizens, regardless of their resources or personal characteristics (Schur et al. Reference Schur, Shields, Kruse and Schriner2002). If our results point to a biasing effect of depression on decision‐making processes in this referendum, that is not an argument against either the legitimacy of those decisions or the use of referendums. Rather, it has one specific and one general implication. The first, familiar from assessments of this and many other electoral contests, is that politicians should not seek to capitalise on or exploit such sensitivity to risk. The second is that campaigns should be structured – and perhaps even regulated – in a way that caters for various types of limitations in political judgement. The fact that these demands sound aspirational, even utopian, does not blunt their normative point.
Acknowledgements
We are thankful to Understanding Society, especially Jay James and Nicole Martin, for accepting our research proposal within the EURef application and granting us early access to the EU Referendum data. We also thank Stuart Fox, Jennifer Hampton, Esther Muddiman, Chris Taylor and the other participants at the EURef events as well as Mikko Mattila, Achillefs Papageorgiou, Lauri Rapeli and Pat Corrigan for their feedback in the initial stages of this project. We apologise to anyone else we might be missing. Finally, we thank the four anonymous reviewers and the editor for their comments.
Online Appendix
Additional supporting informationmay be found in theOnlineAppendix section at the end of the article:
Table S1. Analysis with Mental Component Summary
Table S2. Socio‐political determinants of clinical depression (Understanding Society, Wave 1)
Table S3. Summary statistics
Figure S1. Effects over time of Mental Health (good, medium, poor) on the probability of supporting Brexit





 Open access
Open access