

Introduction
Compared to urban populations, individuals living in rural areas experience greater disparities in chronic conditions and health care access including digital access [Reference Anderson, Saman, Lipsky and Lutfiyya1–Reference Golembiewski, Gravholt and Torres Roldan6]. The Center for Clinical and Translational Science (CCaTS) Rural Health Research Core focuses on community-engaged research to address the challenges posed by geographical and digital barriers to healthcare access and delivery. Central to this initiative, we formed a Midwest Rural Health Research Community Advisory Board (CAB), which includes members of the public living or working in rural areas of Minnesota, Wisconsin, and Iowa. The CAB serves to amplify the voices of rural community members, play a crucial role in advising on research and educational initiatives, and foster strong researcher-rural community relationships.
Past research has established involving CABs in the research process addresses relevant local health needs [Reference Patten, Albertie and Chamie7] and researchers benefit from CAB involvement [8] across all stages of the translational science spectrum [Reference Brockman, Shaw and Wiepert9,10]. Assessing the CAB’s influence across specific stages of research can help identify the strengths of community-engaged research and highlight areas where the CAB’s contributions to the research process could be further developed [Reference Brockman, Balls-Berry and West11]. In this report we used mixed methods to evaluate how researchers perceived the feedback received from the Midwest Rural Health Research CAB as contributing to various aspects of the rural health research process.
Methods
The Mayo Clinic Institutional Review Board approved this project. Data were collected in and analyzed in 2023–2024.
CCaTS Rural Health Research Core (RHRC)
Mayo Clinic’s CCaTS has a long history of community engagement with local populations and has an established CAB at each location in Rochester, MN, Phoenix, AZ, and Jacksonville, FL [Reference Patten, Albertie and Chamie7]. New to CCaTS in 2022 is the Rural Health Research Core (RHRC), which focuses on Rochester and the community-based Mayo Clinic Health System (MCHS) [12] practice that spans counties in Minnesota, Wisconsin, and Iowa. Approximately 66% of MCHS patients live in rural areas compared to about 16% of the general US population [Reference Bank13]. The RHRC is designed to address rural community needs around health care access, including digital access.
Midwest Rural Health Research CAB
The CAB was formed in 2023. Members engage bidirectionally with Rural Health RHRC staff and researchers to co-design, guide, and facilitate rural community-based research projects and educational efforts in the Midwest (Rochester and MCHS). In 2023, the CAB included sixteen members, comprising individuals who lived and/or worked in rural areas, who reported having a close connection to their local rural community and a local rural community perspective. CAB members were diverse with respect to age, gender, racial/ethnic identities, and disability status as well as lived experience. The diversity of the CAB was determined through information shared by CAB members in the orientation meeting and at CAB meetings as relevant to the topic presented. However, demographic information was not collected in a systematic manner for reporting purposes.
Meeting process
The CAB convened quarterly meetings and held nine ad hoc meetings in 2023. The ad hoc meetings were held in response to researchers’ interest in presenting to the CAB that could not be accommodated at the scheduled quarterly meetings. All meetings followed the same structure. A total of thirteen researchers presented their work addressing rural health access (n = 3), digital access and equity (n = 3), cancer (n = 3), cardiovascular disease (n = 2), and diabetes (n = 2). Delivered via Zoom, presentations and discussions typically lasted around 30–50 minutes, with 15–20 minutes allocated for the presentation and 15–30 minutes reserved for discussion with CAB members.
Researchers used PowerPoint slides. The CAB coordinator met with the researchers approximately one month before the presentation to help them prepare and ensure the slides and any materials presented were appropriate for a lay audience. Researchers were asked to share a brief project summary, timeline, future plans to share data and findings, and 1–4 key questions for CAB input. Researchers were advised to avoid technical jargon and limit the use of statistics and acronyms. Slides (maximum of 15) and any handouts were to be submitted at least one week in advance for CAB member review.
Each meeting was facilitated by the CAB coordinator, who guided discussion between the researchers and CAB members to ensure a respectful, inclusive space that encouraged participation and feedback from all CAB members, while also keeping the meeting on schedule. Meetings were recorded. The CAB coordinator wrote a summary of all comments made during the meeting; non-verbal interactions were not documented. The summary was provided to researchers by email within 1–2 weeks after the meeting. CAB members were offered an honorarium of $50 to attend each meeting.
Researcher evaluation
From February 2024 to April 2024, these 13 researchers were invited by email to complete the Community Stakeholder Impact on Research Taxonomy measure, a structured, 7-item, quantitative survey measuring CAB influence defined as community contributions to the research process (Supplement Material) [Reference Stallings, Boyer and Joosten14]. Researchers were asked “In what ways did the feedback from the CAB influence your research?” across seven key research domains: (1) pre-research activities, (2) research infrastructure, (3) study design, (4) implementation, (5) data analysis, (6) dissemination of results, and (7) post-research activities. Examples were provided for each domain. Researchers responded Yes or No to each of the 7 domains. The taxonomy was developed through extensive qualitative work with researchers and community members (i.e., expert reviews) and the preliminary analysis codes were confirmed in a sample dataset [Reference Stallings, Boyer and Joosten14]. Respondents were provided the opportunity for open-ended responses, “Describe how the feedback you received from the CAB members influenced your research project.” Findings were shared with CAB members for results interpretation and input on next steps.
Quantitative and qualitative analyses
Quantitative analysis
SPSS software was used to calculate descriptive statistics (frequencies, percentages) for endorsement of each of the seven domains. An overall mean score was also calculated by summing the number of domains endorsed and averaging across all respondents (possible range: 0–7; higher scores indicate greater influence).
Qualitative analysis
Using conceptual content analysis [Reference Krippendorff15], to identify themes from researchers’ open-ended responses, two authors (TAB, ES) independently coded data using an iterative process via excel software. Using pre-determined categories based on each domain of impact, themes were generated and any discrepancies were discussed with a third author (CP) until consensus was reached. We did not conduct member checking [Reference Krippendorff15]. CAB members’ feedback was summarized.
Results
Eleven of the 13 researchers who presented (85%) completed the post CAB meeting survey. All 11 reported at least one domain where the CAB feedback contributed to their research. Of the 11 respondents, 4 endorsed three domains that were influenced, 3 endorsed two domains influenced, and 1 each endorsed four, five, six and seven domains, respectively. When the number of domains influenced was averaged across respondents, the mean was 3.64 (range 2–7).
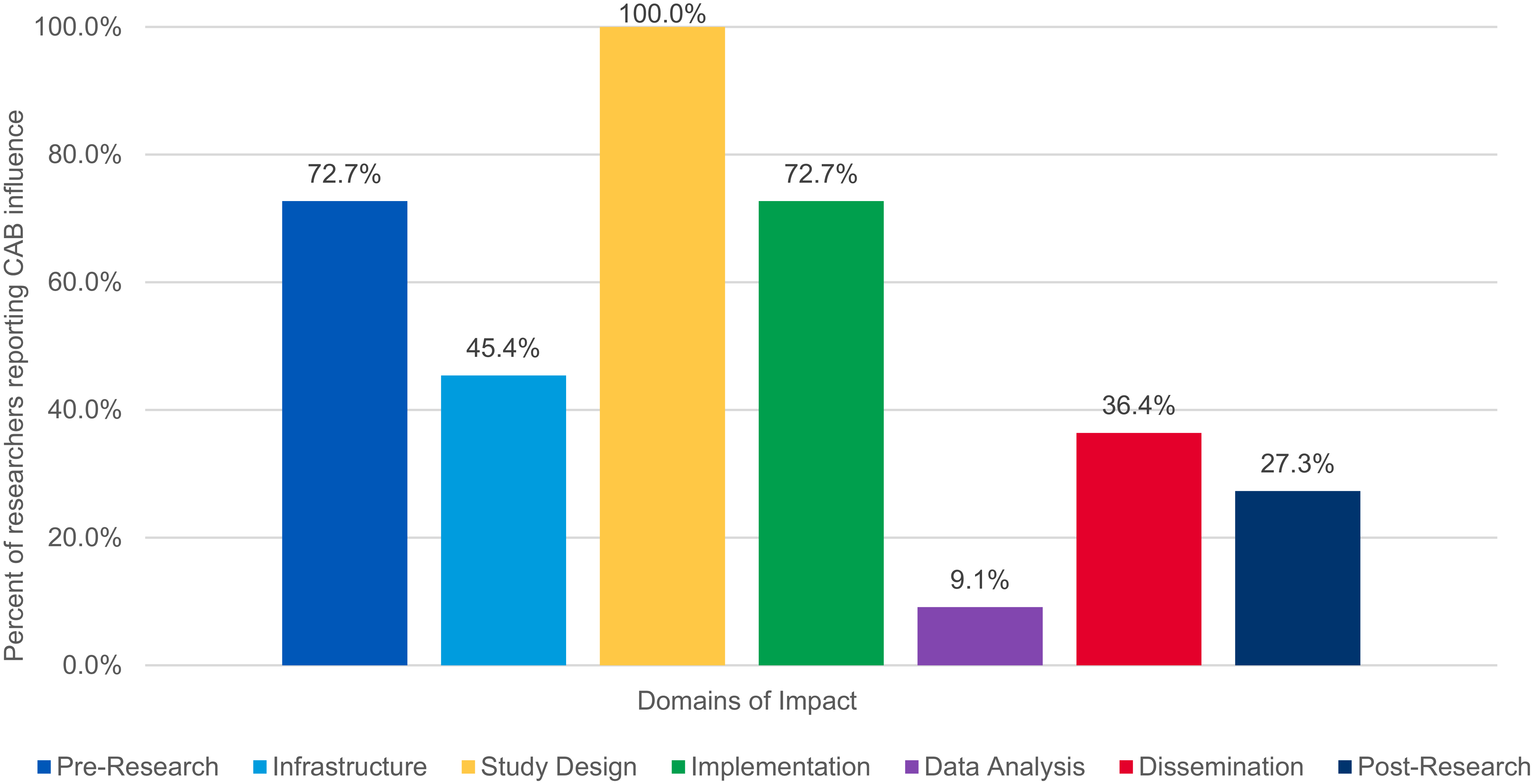
Figure 1 shows the percentage of researchers reporting CAB influence across the 7 domains. The largest reported influence of CAB feedback was on study design (100%; 11/11), followed by pre-research activities (73%; 8/11), and implementation (73%; 8/11). Less than half of the sample endorsed CAB influence on research infrastructure (45%; 5/11), dissemination (36%; 4/11), post-research activities (27%; 3/11), and data analysis (9%; 1/11). The mean total influence score was 3.6 (SD = 3.06, range 0–7) of a possible 7.0.

Figure 1. Influence of midwest rural health research CAB feedback on research domains in 2023 from survey of N = 11 researchers.
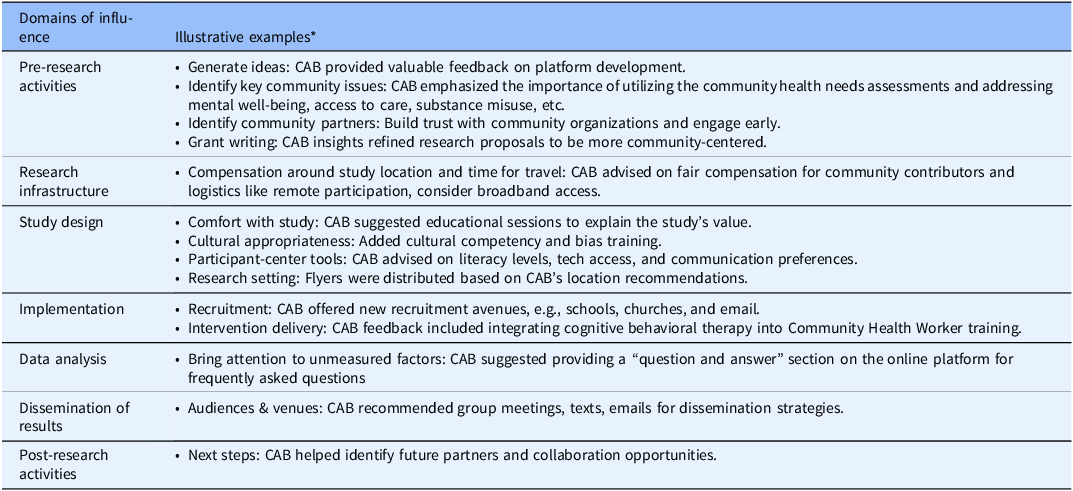
All 11 researchers provided at least one open-ended response. Open-ended responses highlighted major themes of CAB contributions, including generating ideas, patient-centered intervention design and recruitment strategies, and dissemination (Table 1). Some researchers expressed that the CAB brought issues or ideas to their attention that they otherwise would not have considered, especially in terms of study design and recruitment efforts. One researcher remarked, “This was so very valuable for me! CAB members helped me think about various recruitment avenues I hadn’t considered (schools, FFA groups, churches). This has proven incredibly fruitful and useful!” Additionally, CAB feedback prompted specific changes, such as modifications to interview questions and exploring alternative communication methods for recruitment. One researcher noted:
Table 1. Illustrative examples of ways researchers reported the Midwest Rural Health Research Community Advisory Board (CAB) feedback influenced their research across the 7 research domains

Note: *Examples included within each domain are from unique respondents.
“Specific questions were changed in our interview guide because of their feedback. They (CAB) also recommended an alternative form of communication for recruitment of potential candidates (email), which we have not yet explored but I was surprised to find that it would likely be a successful, or at least welcome, strategy for recruitment.”
CAB input was also instrumental in refining research proposals to better align with target population characteristics and ensure continued compliance with research protocols. As one researcher stated, “It was valuable information to refine our research proposal to make it more population centered.” The CAB’s suggestions were particularly appreciated during grant writing, with one researcher noting, “We were in the middle of grant writing, their input on community advisory involvement was very helpful. Specifically, their ideas on dissemination and CAB meeting frequency were very appreciated.” The CAB also emphasized building trust, often through ongoing collaboration with community partners, as an essential part of each stage of the research process. One researcher stated, “Rural CAB emphasized the importance of approaching people where they are, build relationships and demonstrating you can be trusted.”
CAB members noted that they appreciated the feedback loop of learning what happened after providing their feedback to researchers and the perceived value of their work. CAB members recommended that researchers: (1) share their experiences with the CAB to highlight its positive contributions, and (2) use visuals to show where CAB feedback is most valuable in research stages to help researchers understand when to engage with the CAB for maximum influence.
Discussion
The Midwest Rural Health Research CAB had substantial reported influence on rural health research by providing feedback that shaped all aspects of the research process. All researchers surveyed reported at least one research domain influenced by CAB feedback, most commonly for study design, pre-research activities, and implementation. Qualitative data in the form of open-ended responses and overarching themes highlighted positive contributions of the CAB’s feedback to each research domain. CAB members drew researchers’ attention to conceptual and practical considerations for their studies that benefited their research which may have been missed without community input. Integrating the unique perspectives of community members into the research process fostered improvements in each research stage. CAB members appreciated learning about the influence their feedback had on the research projects and valued seeing how their contributions shaped the research in rural communities.
In areas where the domain of influence was under 50%, CAB members thought it was essential to raise awareness among researchers about the value of engaging the CAB early in the process. For example, data analysis is a pivotal phase where hypotheses are tested, and questions are refined. CAB members can play a valuable role in this stage by offering alternative interpretations of the data even before the data is collected. Their input can help shape the direction of the research, ensuring that the analysis reflects diverse perspectives and is more robust in its findings.
One strategy identified by the CAB was that researchers who have worked with a CAB share their experiences to emphasize its contributions, specifically through visuals that show where CAB feedback is most helpful in the research process. Spreading the word about the benefits of working with a CAB could enhance CAB engagement, particularly in underutilized research domains, such as data analysis, research infrastructure, dissemination and post-research activities. Leveraging the illustrative examples from Table 1 and other experiences we have advising researchers, we plan to create an infographic presentation of all the domains (with examples) and share that with researchers prior to the planning meeting so they are primed to think about all the areas in which the CAB could offer feedback. Sharing results back with the CAB, specifically how their feedback was utilized, is an expectation of researchers presenting to the CAB. The CAB coordinator follows up with researchers within 6 months of their presentation and then schedules a time for sharing back with CAB members. CAB members appreciate this feedback loop. CAB members also suggested it may be beneficial to offer training to CAB members to deepen their knowledge and understanding in domain areas that were less influenced, empowering them to provide more helpful feedback. It would be valuable to explore whether CAB members perceive their investment of time in training as worthwhile, including whether they feel their contributions meaningfully shape rural healthcare research outcomes and decision-making.
CAB contribution to the research process is most often evaluated through surveys assessing general engagement and satisfaction of CAB members and/or researchers [Reference Matthews, Anderson, Willis, Castillo and Choure16–Reference Wallerstein, Ward, Boursaw, Eder, Kastelic and Oetzel19]. Prior reports focused on evaluating the contributions of CAB feedback to the research process [Reference Brockman, Balls-Berry and West11–Reference Stallings, Boyer and Joosten14] but our study adds to the literature by its focus on such contributions to rural health research. The combination of quantitative and qualitative measures offered a more in-depth understanding of the CAB’s influence than could be provided by either alone. Further, the variety of health topics presented by researchers included in this study demonstrates CABs’ ability to contribute to a range of rural health research. However, this evaluation is limited by the small sample size (n = 11), a focus on short-term contributions to the research process, and lack of data collected on CAB member demographics/representation or other mediating factors that may have contributed to the results. Thus, the findings are considered preliminary. Moreover, the evaluation was done in a Midwest setting, limiting generalizability to other rural contexts.
Future steps include a fuller evaluation of CAB contributions to the research process within our setting which could be used as a framework across the CTSA consortium. For example, with a larger sample size, evaluation of CAB influence could be summarized by health topics presented by investigators to explore if CAB contributions vary based on the types of rural health research. Self-reported data as well as publicly available data (e.g., PubMed, NIH Reporter) could be collected on longer term outcomes such as successful study implementation, funding of submitted grants, and publications. Different use cases or stories of short and long-term influence on the research process could also be shared across the CTSA consortium to collectively tell the story of community engagement through CAB platforms.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/cts.2025.10225
Acknowledgements
We wish to thank the members of our Midwest Rural Health Research CAB for their time, dedication, involvement, and partnership with the Mayo Clinic, which is vital to the development of meaningful research, as well as researchers for their participation and contributions. We would also like to thank Kimberly Kinnoin for manuscript assistance.
Author contributions
Tabetha A. Brockman: Conceptualization, Data curation, Formal analysis, Methodology, Project administration, Writing-original draft, Writing-review & editing; Audrey McGuinness: Formal analysis, Writing-original draft, Writing-review & editing; Julie T. Elworth: Formal analysis, Writing-review & editing; Emily Sabey: Data curation, Formal analysis, Writing-review & editing; Rebeca Sedarski: Formal analysis, Writing-review & editing; Sara Lee: Formal analysis, Writing-review & editing; Carolyn Petersen: Formal analysis, Writing-review & editing; Jerry Clark: Formal analysis, Writing-review & editing; Beth Breeden: Formal analysis, Writing-review & editing; Christi A. Patten: Conceptualization, Formal analysis, Methodology, Project administration, Writing-original draft, Writing-review & editing.
Funding statement
This project was supported by the National Center for Advancing Translational Sciences (grant number UL1 TR002377). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH.
Competing interests
The author(s) declare none.



 Open access
Open access