


Major depression represents a pervasive challenge within our society. The World Health Organization rated major depression as the third leading cause of the global burden of disease in 2008. 1 In 2019, approximately 280 million individuals worldwide suffered from a depressive disorder, reflecting a prevalence of 3.8% in the global population. The prevalence of depression is higher in some age groups, with rates of 5.0% in adults aged 20 years and ranging from 5.2 to 5.8% in adults aged 40–69. 2 Gender differences further compound this issue, because women are around twice as likely as men to develop a depressive episode, a divide that is apparent from young adulthood to the post-menopausal stage. Reference Sassarini3
The consequences of depressive disorders extend beyond individual suffering, impacting family, friends and the workplace. In severe cases, these can lead to suicidal thoughts and actions, with depression being a prominent factor in approximately 800 000 global suicides in 2015. Reference Bachmann4 In addition to the individual effects and reduced quality of life, depression also exacts an economic toll through reduced productivity and an increase in both sick leave days and direct costs. Reference König, König and Konnopka5
Considering the time that adults dedicate to work, it becomes imperative to identify work-related risk factors for the development and persistence of a depressive disorder. Because middle-aged individuals primarily drive our economy, prioritising their long-term health is critical. Simultaneously, given its pivotal role, we must address whether the workplace significantly impacts their mental health. In a meta-analysis published in 2005, it was elucidated that job dissatisfaction is significantly associated with mental disorders, particularly burnout and depression. Reference Faragher, Cass and Cooper6 Another recent meta-analysis has also shown a correlation between job strain and clinical depression. Reference Madsen, Nyberg, Magnusson Hanson, Ferrie, Ahola and Alfredsson7 Despite considering the factors influencing job satisfaction – such as income, working hours, workload and interpersonal dynamics – the most recent literature largely fails to account for other relevant aspects, such as subjective under- or overload given the qualifications required for the work. Only a few studies have addressed subjective challenges. Reference Lehmann, Burkert, Daig, Glaesmer and Brähler8 Recent meta-analytic evidence from a comprehensive global review of healthcare professionals highlights the significant and multifaceted relationships among job stress, low job satisfaction, workplace bullying and burnout, emphasising the importance of addressing both workload- and qualification-related challenges in occupational health research. While this meta-analysis almost exclusively includes cross-sectional and case-control studies that provide snapshots of associations between occupational stress and outcomes such as burnout, these designs cannot establish temporal sequences or causality and may be influenced by transient circumstances or confounding factors. Reference Sohrab Amiri, Mustafa, Javaid and Khan9 The majority of studies examining job satisfaction, as well as the limited research on subjective overload and under-challenge in association with depressive symptoms, adopt a cross-sectional and observational design. Reference Franks, Chen, Manley and Higgins10,Reference Weigl, Stab, Herms, Angerer, Hacker and Glaser11
For example, a cross-sectional study published in 2011 showed an association between subjective under-challenge and depressive symptoms. Reference Lehmann, Burkert, Daig, Glaesmer and Brähler8 Another study, based on cross-sectional data, showed that mental health could be damaged by either too many or too few challenges compared with exactly the right level of challenges. Reference Franks, Chen, Manley and Higgins10
To date, there is very restricted evidence regarding the association between self-rated under-challenge or overload at work and depressive symptoms. The studies mentioned above are restricted in their cross-sectional design, which makes it challenging to elucidate causality and directionality. However, they point to the importance of studying depressive symptoms more closely in connection with work-related factors. It is crucial to examine the complex relationship between the challenge levels in occupational settings and the manifestation of depressive symptoms. Given the absence of findings based on longitudinal data, this study aims to examine longitudinally, among middle-aged individuals, the association between subjective overload or under-challenge, given one’s qualification for the occupation, and the occurrence of depressive symptoms.
Understanding the potential link between inadequate subjective challenge at work and depressive symptoms may help to identify middle-aged individuals at risk for depression longitudinally, and thus the opportunity to intervene early. By employing a longitudinal analytic framework, this study allows for temporal inferences and captures intra-individual change, marking a methodological advancement over previous cross-sectional designs.
Method
Sample
This study utilised data gathered from waves 3 (2008), 4 (2011), 5 (2014) and 6 (2017) of the cross-sectional and longitudinal German Ageing Survey (DEAS). The survey was initiated in 1996 by the Research Data Centre of the German Centre of Gerontology (DZA), funded by the Federal Ministry for Family Affairs, Senior Citizens, Women and Youth. The survey sampled Germans registered within municipalities and who are in their ‘second half of life’, aged 40 years and above. Employing a cohort-sequential design, DEAS introduced new baseline samples approximately every 6 years (in waves 2 in 2002, 3 in 2008 and 5 in 2014); since 2008, the DEAS panel has been surveyed every 3 years. Reference Klaus, Engstler, Mahne, Wolff, Simonson, Wurm and Tesch-Römer12,Reference Engstler, Stuth, Lozano Alcántara, Luitjens, Klaus and Schwichtenberg-Hilmert13
The DEAS study enrolled individuals through a national probability sampling to ensure representative inclusion. The adults included in the survey are a sample based on a random selection of 290 municipalities drawn in 1996 from the total of 12 000 municipalities that existed in Germany at that time. Each baseline year, the local population registries of these 290 municipalities served as the basis for sampling individuals aged between 40 and 85 years and who lived in private households within the community. The DEAS survey covers various topics such as socioeconomic circumstances, family dynamics, work and retirement, health-related aspects and age transition. The data were collected through standardised questionnaires administered by trained interviewers and self-administered written questionnaires. The participants in each wave were invited to complete future waves, ensuring longitudinal data. Reference Klaus, Engstler, Mahne, Wolff, Simonson, Wurm and Tesch-Römer12,Reference Engstler, Stuth, Lozano Alcántara, Luitjens, Klaus and Schwichtenberg-Hilmert13 To reduce attrition, DEAS reduced the interval between panel waves from 6 to 3 years from 2008 onwards, and thus we have focused on the waves from 2008 until the beginning of the COVID-19 pandemic to ensure the highest possible follow-up. In 2008, a total of 17 366 individuals were eligible for inclusion and the response rate was 35.7%. The retention rate from the baseline year (2008) to the survey year (2011) was, for example, 46.1%, and the retention rate from 2008 to 2014 was 41.4%. Please see the DEAS Cohort Profile for further details. Reference Klaus, Engstler, Mahne, Wolff, Simonson, Wurm and Tesch-Römer12
Due to the COVID-19 pandemic and the subsequent shifts in social and work behaviour – as well as the effects on mental health – we relied on data from waves 3–6, gathered before the onset of the pandemic and capturing all relevant variables. This study employed linear fixed-effects regressions to investigate intra-individual variable changes over time (please see Statistical analysis, below, for further details). Our analytical sample included 7487 observations from 4362 individuals. Stratified by gender, our analysis includes 3668 observations corresponding to 2169 individuals among males, and 3819 observations corresponding to 2193 individuals among females.
The DEAS study followed the Declaration of Helsinki but did not require an ethical declaration because the prerequisites were unmet. Because no ethics vote was needed, according to the German Research Foundation, DZA did not pursue one. All data were collected, anonymised and processed in accordance with strict data protection regulations, to protect participants when working with sensitive mental health information. For further information on DEAS, including methodology, data, findings and related publications, please visit the DZA homepage. Reference Klaus, Engstler, Mahne, Wolff, Simonson, Wurm and Tesch-Römer12,14
Dependent variable
As the dependent variable, we analysed the depressive symptoms of study participants using a 15-item version of Radloff’s Center for Epidemiologic Studies Depression Scale (CES-D). Reference Radloff15,Reference Hautzinger, Bailer, Hofmeister and Keller16 CES-D is a self-report measure of depression with a range in scores of 0–45, with higher values reflecting more depressive symptoms. The participants were asked 15 questions about their feelings and thoughts over the past week. Each item ranged on a 4-point scale: 1 = rarely or not at all (<1 day); 2 = sometimes (1−2 days); 3 = occasionally or a moderate amount of time (3−4 days); and 4 = most or all the time (5−7 days). Reference Shaffer and Michalos17
Independent variable
This study employed a single item to assess subjective under-challenge and overload within the context of participants’ occupations. Participants were asked to evaluate their perceived job adequacy concerning current work demands using the statement: ‘Do you think that you are properly qualified for your job, given the current demands of your work? In view of your qualifications, do you feel…’ Responses were rated on a scale ranging from 1 (under-challenged) to 3 (overloaded). Reference Engstler, Stuth, Lozano Alcántara, Luitjens, Klaus and Schwichtenberg-Hilmert13 Given the absence of standardised psychometric instruments for quantification of this construct, we utilised the question above to measure subjective under- and overload at work-given qualification. This methodology resonates with similar formulations in multiple questionnaires designed to assess workplace stressors, e.g. ‘Mental stress – recognising and eliminating risks’. Reference Richter, Friesenbichler and Vanis18
Covariates
In alignment with previous research, Reference Sassarini3,Reference Ambresin, Chondros, Dowrick, Herrman and Gunn19–Reference Gutiérrez-Rojas, Porras-Segovia, Dunne, Andrade-González and Cervilla22 we selected and adjusted for different time-varying covariates. In terms of socioeconomic factors, these were adjusted for age (years), marital status (single, divorced, widowed, married and living separated from spouse, married and living together with spouse), as well as net household income (in euros). Regarding health-related factors, we adjusted for self-rated health, a subjective measure of a person’s overall health status (ranging from 1 = very good to 5 = very bad). Moreover, we adjusted for a count of chronic diseases (ranging from 0 to 11), including cardiac and circulatory disorders; bad circulation; joint, bone, spinal and back issues; respiratory concerns; stomach and intestinal problems; cancer; diabetes; gall bladder, liver and kidney problems; urogenital problems; eye or vision impairment; and ear or hearing problems.
We used the time-constant factor of gender (men/women) to stratify the linear fixed-effects regressions. For descriptive purposes, we utilised education levels categorised according to the International Standard Classification of Education (ISCED-97), distinguishing between low (0–2), medium (3–4) and high (5–6) levels of education. 23
Statistical analysis
We performed all statistical analyses using Stata version 17.0 for Windows (StataCorp LLC, College Station, Texas, USA; https://www.stata.com), with statistical significance set at P < 0.05. To characterise the data, we conducted descriptive statistical analyses then investigated the correlation of our variables and analysed longitudinal patterns. Therefore, we employed multiple linear fixed-effects regressions to investigate the longitudinal association between the perceived occupational challenge and the occurrence of depressive symptoms. Because both perceived occupational challenges and depressive symptoms were measured in the same survey wave, it cannot be definitively determined whether overload precedes depressive symptoms. In the fixed-effects regressions, we adjusted for the identified time-varying covariates. Reference Gutiérrez-Rojas, Porras-Segovia, Dunne, Andrade-González and Cervilla22
Fixed-effects regression is commonly used in panel data analysis to include changes within individuals over time, such as in occupational challenges, from one wave to another. The main advantage of fixed-effects regression is that it can provide consistent estimates even when time-constant factors – observed and unobserved – are associated with predictors. Reference Cameron and Trivedi24 Consequently, only time-varying factors, such as self-rated health or chronic disease count, can be utilised as explanatory variables in fixed-effects regressions as main effects. Because time-constant factors, such as gender, cannot be used as main effects, we stratified the fixed-effects regression by gender.
Results
Sample characteristics
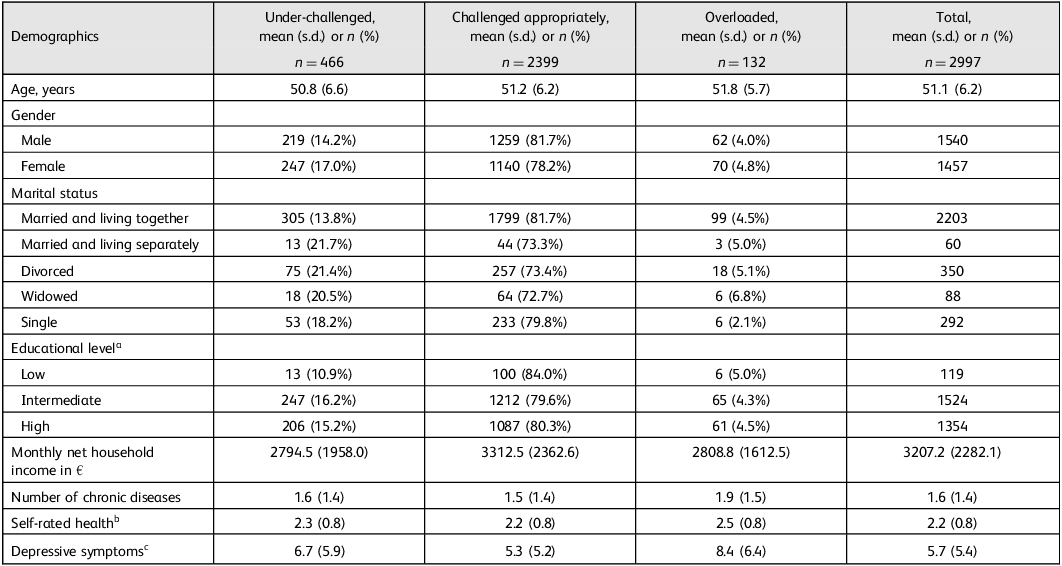
In total, 4362 individuals were included in the study. For those surveyed in 2008 alone (n = 2997), their characteristics are outlined in Table 1. The average age was 51.1 years (s.d. 6.2), ranging from 40 to 64 years. Of these individuals, 1540 (51.4%) were male. At baseline, 2203 (73.6%) participants reported being married and living with a spouse. Most participants had an intermediate level of education (50.9%, n = 1524), followed by a high level (45.2%, n = 1354), while a minority had a low educational level (4.0%, n = 119). The monthly mean net household income of study participants (in euros) was 3207.2 (s.d. 2282.1). On average, individuals had 1.6 chronic diseases (s.d. 1.4) and self-rated health was 2.2 (s.d. 0.8). The mean score for depressive symptoms was 5.7 (s.d. 5.4). Further details can be found in Table 1.
Table 1 Overload and under-challenge in occupation: baseline characteristics

a. The International Standard Classification of Education (ISCED-97) provides a framework for the categorisation of educational status, achievements and qualifications into internationally recognised levels, ranging from 0 to 6. A person with ISCED 0–2 is considered to have a low level of education, while ISCED 3–4 is intermediate and ISCED 5–6 is high. 23
b. Self-rated health is a subjective measure of a person’s overall health status, ranging from very good (1) to very bad (5). Reference Engstler, Stuth, Lozano Alcántara, Luitjens, Klaus and Schwichtenberg-Hilmert13
c. The Center for Epidemiological Studies Depression Scale (CES-D) is a self-report measure of depression with a scoring range of 0–45, with higher values reflecting more depressive symptoms. Reference Shaffer and Michalos17
Regarding feelings of being under-challenged, 247 women (53.0% of all under-challenged participants) reported such sentiments, compared with 219 men (47.0%). Conversely, 70 women (53.0%) and 62 men (47.0%) reported feeling overloaded. Most participants – 1140 women (47.5%) and 1,259 men (52.5%) – perceived the challenge level in their occupation as exactly right.
Regression analysis
Total sample
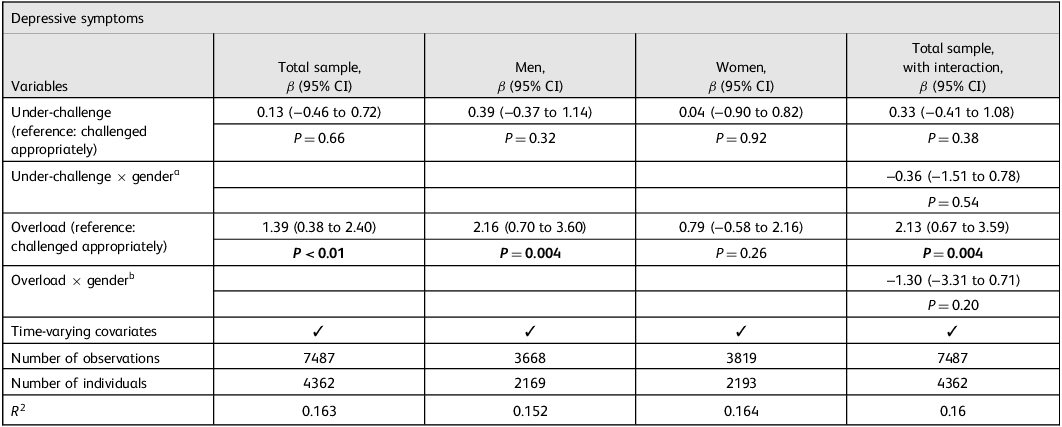
The results of multiple linear fixed-effects regressions are shown in Table 2 (total sample; stratified by gender; and with interaction terms). Intra-individual transitions, from ‘challenged appropriately’ to ‘under-challenged’ for occupation were not significantly associated with changes in depressive symptoms. In contrast, intra-individual transitions from ‘challenged appropriately’ to ‘overloaded’ were significantly associated with increases in depressive symptoms (β = 1.39, 95% CI: 0.38 to 2.40, P < 0.01).
Table 2 Linear fixed-effects regression, with occupational challenge as the dependent variable and depressive symptoms over time, adjusting for potential time-varying covariates

Results of linear fixed-effects regressions with unstandardised β coefficients. Time-varying covariates include age, marital status, net household income, self-rated health and a count of chronic diseases; ‘×’ denotes interactions.
a. Interaction term 1: women (reference: men) × under-challenged (reference: challenged appropriately).
b. Interaction term 2: women (reference: men) × overloaded (reference: challenged appropriately).
P-values in bold indicate statistical significance **P < 0.01.
Stratified by gender
When stratified by gender, intra-individual transitions from ‘challenged appropriately’ to ‘under-challenged’ for occupation were not significantly associated with changes in depressive symptoms among male individuals (β = 0.39, 95% CI: −0.37 to 1.14, P = 0.32). However, intra-individual transitions from ‘challenged appropriately’ to ‘overloaded’ among men were significantly associated with changes in depressive symptoms (β = 2.16, 95% CI: 0.70 to 3.60, P = 0.004).
Among women, the average within-person change from ‘challenged appropriately’ to ‘under-challenged’ was not significantly associated with changes in depressive symptoms (β = 0.04, 95% CI: −0.90 to 0.82, P = 0.92). Intra-individual transitions from ‘challenged appropriately’ to ‘overloaded’ among female individuals were also not significantly associated with changes in depressive symptoms (β = 0.79, 95% CI: −0.58 to 2.16, P = 0.26). The corresponding interaction terms (occupational challenge × gender) did not achieve statistical significance. Please see Table 2 for further details.
Discussion
This longitudinal study aimed to investigate the association between subjective work challenges and depressive symptoms – also stratified by gender – using a fixed-effects regression model. Our research extends the very few existing cross-sectional studies by utilising longitudinal data from a large, nationally representative sample. Our key findings revealed that intra-individual transitions from being appropriately challenged to overloaded in the ‘occupation, given job qualification’ were significantly associated with increased depressive symptoms among the total sample. Even moderate increases in depressive symptoms can affect daily functioning and work performance, highlighting the importance of addressing overload in the occupation. Our study found similar associations between overload and depressive symptoms among men, but not among women, whereas intra-individual transitions from being appropriately challenged to under-challenged were significantly associated neither with changes in depressive symptoms in the total sample, nor when stratified by gender. Although significant research has been conducted on the relationship between job dissatisfaction or job strain and the risk of psychological diseases, it remains unclear how completion of tasks for which workers do not feel qualified impacts the development of these diseases. Several studies have found that low job satisfaction is significantly linked to depressive symptoms and anxiety. Reference Faragher, Cass and Cooper6 Job satisfaction is measured mainly by either a single-item question or assessing an employee’s satisfaction with various job components, such as whether they find their job interesting, have good relationships with managers and colleagues, receive a high income, have the freedom to work independently and have clear career advancement opportunities. Reference Faragher, Cass and Cooper6,Reference Saquib, Zaghloul, Saquib, Alhomaidan, Al-Mohaimeed and Al-Mazrou25–Reference Niedhammer, Malard and Chastang27 Individuals experiencing high job strain – which is characterised by high demands and low work control – are also more likely to develop clinical depression. Reference Madsen, Nyberg, Magnusson Hanson, Ferrie, Ahola and Alfredsson7 The Swedish Demand-Control-Support Questionnaire (DCSQ) is a validated tool often used to study job strain. Reference Mauss, Herr, Theorell, Angerer and Li28 However, this questionnaire does not include questions regarding psychological demands based on qualifications. Although overload can be considered a factor for increased job strain, the DCSQ does not cover this. Nonetheless, our findings linking overload to depressive symptoms suggest that it could be considered a component of increased job strain, supporting the evident association between job strain and depression. Even if challenges stemming from professional qualifications are regarded as a component of psychological demands, examining these as an independent variable remains valuable. Despite some studies incorporating high demand or work overload into their composite outcomes, none have explored challenges because of over- or under-qualification as distinct factors. Reference Faragher, Cass and Cooper6,Reference Madsen, Nyberg, Magnusson Hanson, Ferrie, Ahola and Alfredsson7,Reference Weigl, Stab, Herms, Angerer, Hacker and Glaser11 These, however, might particularly affect the negative work-related stress and, thus, the occurrence of depression. For instance, while high demands may not necessarily be stressful for a well-qualified and satisfied worker, they could become distressing if coupled with feelings of under-qualification. We recommend future research to examine this in more detail.
Our study results are particularly interesting in light of the gender-specific differences found; the non-significant interaction may be explained largely by a lack of statistical power. The literature suggests that women have a more inadequate stress adaptation and a higher prevalence of depressive disorders. Reference Sassarini3,Reference Karamihalev, Brivio, Flachskamm, Stoffel, Schmidt and Chen29 One possible explanation is that when work is considered more critical for one’s satisfaction and fulfilment in life than in other areas, the absence of such satisfaction can significantly affect one’s mental health. Reference Saunders and Roy30 Recent data indicate that female employment in Germany has increased in the past few years, resulting in a decrease in gender-based disparities in employment ratios. Nevertheless, women tend to be employed in part-time jobs more frequently than men, which means that men still work more hours overall. Reference Ilieva and Wrohlich31 As a result, men may view work as a more central aspect of their lives than women. Reference Reitzes and Mutran32 Therefore, men may also be at a greater risk of experiencing depressive symptoms due to work-related challenges compared with women.
In a Canadian study, researchers discovered that men who deal with high demands and low control at work are more prone to experiencing major depression and anxiety disorders. Reference Wang, Lesage, Schmitz and Drapeau33 Conversely, for women, this specific combination tends to be linked more broadly to various forms of depressive or anxiety disorders. Furthermore, that study highlighted that job insecurity is positively linked with major depression in men, while no such correlation was found among women. Reference Wang, Lesage, Schmitz and Drapeau33 Therefore, one could argue that, if men feel overloaded at work, they may also be at a greater risk for depression due to fear of job loss. Research also indicates that depression among male workers is greater than the national average, especially in male-dominated industries, where rates of depression can vary. Reference Roche, Pidd, Fischer, Lee, Scarfe and Kostadinov34 In this context, breakdown of the areas in which our study participants were employed is also exciting and could be addressed in future studies. In addition, the differences in how men and women cope with work-related stress may also help to explain our research findings. Women tend to use adaptive coping strategies, such as seeking support from family and friends, to deal with stress. On the other hand, men are more likely to use maladaptive and avoidance strategies when faced with stressful situations. Reference Lauren, Jane, Nandar, Stefan, Katie and Jay35 These findings suggest that women adopt healthier and potentially more effective coping mechanisms when dealing with overload at work, compared with men. All the foregoing suggests that unexplored factors such as individual coping strategies, social support networks and variations in stress perception may underlie gender differences. Reference Novais, Monteiro, Roque, Correia-Neves and Sousa36 Therefore, further research must thoroughly examine these variables in future studies.
Our study contradicts one previous study which showed that subjective under-challenge at work is positively associated with depressive symptoms, mediated by life satisfaction. Reference Lehmann, Burkert, Daig, Glaesmer and Brähler8 This relationship between under-challenge and depressive symptoms is consistent across genders in the above study. Other studies indicate a connection only between under-challenge and mood, not depression. Reference Cox, Mackay and Page37,Reference Shirom, Westman and Melamed38 However, conducting further research on this topic is essential to understand better why our longitudinal study produced outcomes different from those of previous cross-sectional studies. One plausible explanation could be that overload may result in longer working hours, whereas individuals experiencing under-challenge may complete their tasks within regular hours, thus affecting differently the perception of stress and its impact on depressive symptoms. Of note, long working hours are positively associated with depressive symptoms. Reference Yin, Ji, Cao, Jin, Ma and Gao39,Reference Weigl, Stab, Herms, Angerer, Hacker and Glaser11
Strengths and limitations
We should consider some of this study’s strengths and limitations when interpreting our current findings. First, this is one of few studies on overload and under-challenge given job qualifications, and their impact on mental health. Second, we used a large, nationally representative sample. Moreover, we utilised longitudinal data and fixed-effects regressions, which significantly reduced the problem of unobserved heterogeneity, a challenge that often arises when using observational data. However, the possibility of reverse causality (i.e. changes in depressive symptoms may also contribute to changes in the perception of occupational challenges) cannot be dismissed. Future research in this area is thus required. We used a single question item to determine whether the participant’s occupation was subjectively overloading or under-challenging, because no validated tools are currently available to measure this variable directly. Although single-item measures may not capture constructs as comprehensively as multi-item scales, research indicates that thoughtfully phrased single items can still provide psychometrically valid evaluations of work stressors. Reference Gwenith, Fisher and Gibbons40 However, all other variables were collected using standardised and validated methods. It is worth noting that the DEAS study has revealed a slight sample selection bias: for instance, participation rates may be lower among residents of large cities. Nonetheless, such effects are minor, and the distribution of sociodemographic characteristics is reasonably similar to that in Germany. Reference Klaus, Engstler, Mahne, Wolff, Simonson, Wurm and Tesch-Römer12
Implications
Based on our study, middle-aged men facing overload at work exhibit higher depressive symptom scores. Efforts to prevent overload may, therefore, be beneficial in avoiding mental health diseases. Although our study did not find heightened depressive symptoms among individuals experiencing under-challenge, there may be implications for efficiency and task allocation. Further research from diverse populations is needed to confirm these findings. Investigation of whether the COVID-19 pandemic had affected work-related challenges would be interesting. Given the significance of family planning in this age group, analysis of work challenges and their association with depressive symptoms among individuals aged 18–39 years, particularly gender-specific differences, is also essential. By addressing work-related stress and reducing overload, we can potentially prevent depression onset, emphasising the importance of supporting individuals at risk.
Data availability
The data used in this study are third-party data. The anonymised data-sets of the German Ageing Survey (DEAS) (1996, 2002, 2008, 2011, 2014, 2017, 2020, 2020/2021, 2023) are available for secondary analysis. The data have been made available to scientists at universities and research institutes exclusively for scientific purposes. The use of data is subject to written data protection agreements. Microdata from DEAS are available free of charge to scientific researchers for non-profitable purposes. The Research Data Centre at the German Centre of Gerontology (DZA) provides access and support to scholars interested in using DEAS for their research. However, for reasons of data protection, signing a data distribution contract is required before data can be obtained. For further information on the data distribution contract, please see https://www.dza.de/en/research/fdz/access-to-data/application (accessed 24 September 2025).
Acknowledgement
We thank the Research Data Centre of DEAS at DZA for providing the data.
Author contributions
P.S.W.: conceptualisation, writing – original draft and preparation, formal analysis, methodology. A.H.: conceptualisation, supervision, validation, writing – reviewing and editing. H.-H.K.: writing – reviewing and editing, supervision, validation. All authors reviewed the results and approved the final version of the manuscript.
Funding
No funding is applicable.
Declaration of interest
None.

 Open access
Open access
eLetters
No eLetters have been published for this article.