


Introduction
Ukraine’s complex security environment, marked by ongoing conflict and threats to critical infrastructure including nuclear facilities, necessitates robust radiological emergency preparedness capabilities.1 The country operates four nuclear power plants with 15 reactors, making radiological preparedness a critical component of national security and public safety.2 Recent global experiences, including the 2011 Fukushima Daiichi nuclear disaster and the 2022 military actions near Ukrainian nuclear facilities, underscore the urgent need for comprehensive emergency response frameworks capable of managing radiological incidents.3
Simulation exercises represent one of the four critical elements of the International Health Regulations (IHR) Monitoring and Evaluation Framework, providing evidence-based assessment of country emergency response capabilities.4 The WHO’s Radiation Emergency Medical Preparedness and Assistance Network (REMPAN) framework emphasizes the importance of regular exercises to test and refine response mechanisms.Reference Carr5 However, regions without nuclear power plants often lack specific radiological emergency preparedness, creating potential vulnerabilities in national response capacity.
The September 2024 tabletop exercise (TTX) conducted by the WHO Ukraine Country Office addressed this gap by testing radiological emergency response capabilities in a region without nuclear facilities but strategically important for national emergency response coordination. The exercise aimed to evaluate 3 critical components: interagency communication effectiveness during radiological emergencies, patient referral pathway efficiency for contaminated casualties, and public information management strategies to counter misinformation and prevent panic.
This assessment was particularly relevant given Ukraine’s current operational environment, where traditional emergency response systems must function under wartime conditions with modified protocols and resource constraints. The exercise provided an opportunity to test adaptability of existing frameworks to radiological scenarios while identifying specific areas requiring enhancement to ensure comprehensive national preparedness.
Methods
Exercise Design and Framework
The TTX employed a structured approach based on established emergency preparedness exercise methodologies, incorporating elements from the WHO REMPAN framework and international best practices for radiological emergency simulation.Reference Hobbs, Lentini and Moran6 The exercise design followed progressive complexity principles, with each inject building upon previous scenarios to test escalating response requirements and interagency coordination under increasing pressure.
Scenario Development
The simulation centered on a catastrophic cooling system failure at the fictional North-West Nuclear Power Plant, designed to avoid security concerns while providing realistic testing conditions. The scenario was developed using technical specifications from actual nuclear incidents, including the Three Mile Island accident progression model, to ensure authentic decision-making challenges.Reference Skryabina, Betts, Reedy, Riley and Amlôt7 The scenario incorporated dose and deposition mapping based on standardized radiological emergency planning zones, with contamination levels ranging from 1 to 3 Gray exposure for plant workers and varying environmental contamination patterns affecting a 30-kilometer radius.
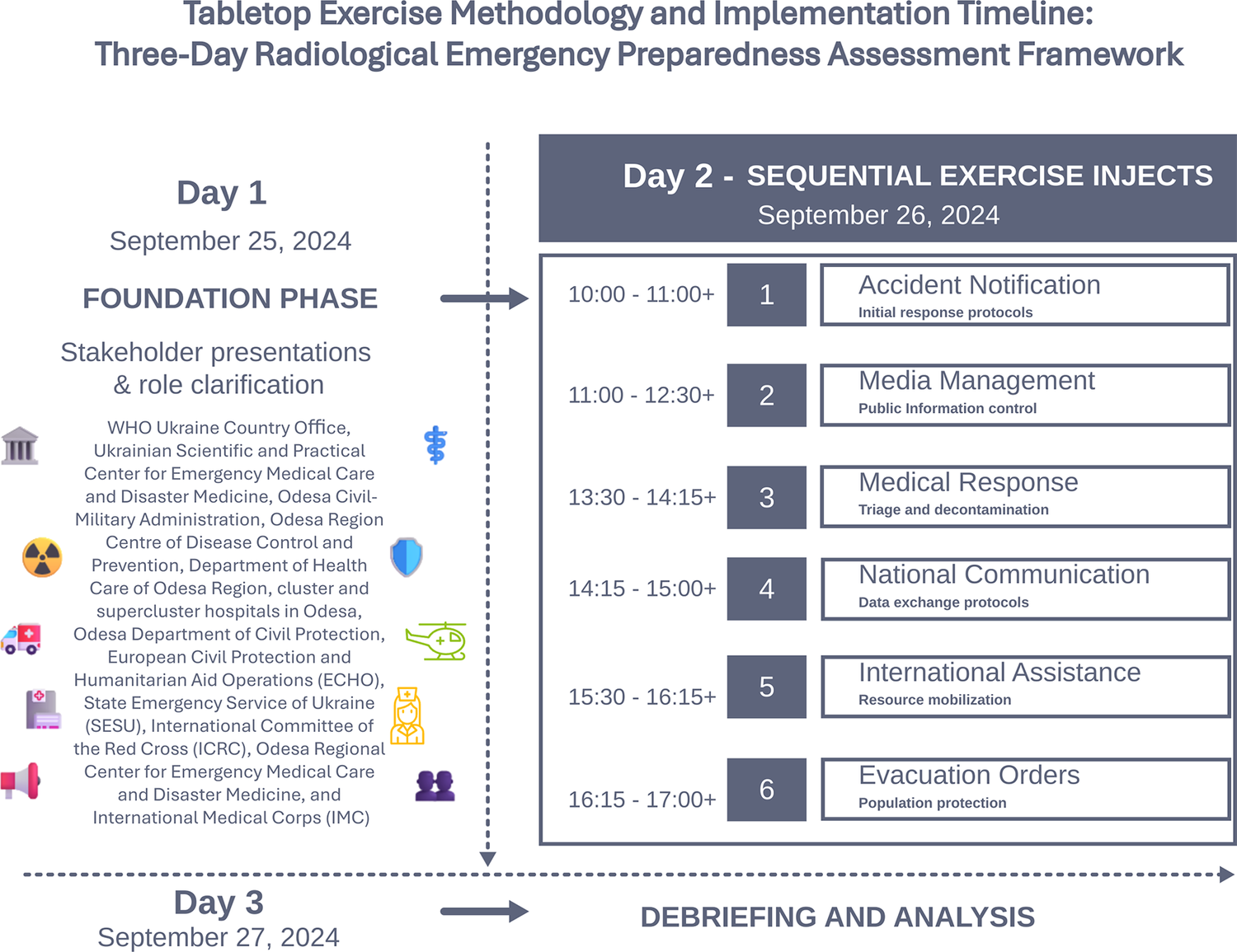
Figure 1 illustrates the 3-day tabletop exercise methodology implemented in September 2024 to assess radiological emergency preparedness capabilities in Ukraine. Day 1 established the foundation through stakeholder presentations and role clarification among 12 participating organizations. Day 2 comprised 6 sequential exercise injects of increasing complexity, testing specific response capabilities from initial accident notification through population evacuation. Day 3 focused on comprehensive debriefing and analysis. The progressive complexity design enabled systematic evaluation of multiagency coordination capabilities while identifying critical preparedness gaps. Icons represent participating organizations including government agencies, health care institutions, emergency services, and international partners.

Figure 1. Tabletop exercise performance assessment: Radiological emergency preparedness capabilities and identified gaps in Ukraine.
Participant Selection and Organizations
Twelve organizations participated, representing the full spectrum of radiological emergency response capabilities: WHO Ukraine Country Office, Ukrainian Scientific and Practical Center for Emergency Medical Care and Disaster Medicine, Civil-Military Administration, Centers of Disease Control and Prevention, Department of Health Care, cluster and supercluster hospitals, Department of Civil Protection, European Civil Protection and Humanitarian Aid Operations (ECHO), State Emergency Service of Ukraine (SESU), International Committee of the Red Cross (ICRC), and International Medical Corps (IMC).
Inject Design and Implementation
Six progressive injects were implemented over 48 simulated hours:
-
1) Accident notification and immediate response, testing initial communication protocols, and rapid response team mobilization;
-
2) Public communication and media management, evaluating misinformation control and public information strategies;
-
3) Medical response and referral pathways, assessing triage, decontamination, and patient transport capabilities;
-
4) Communication with national health institutions, testing data exchange, and coordination mechanisms;
-
5) International assistance and resource mobilization, evaluating integration of external support; and
-
6) Prolonged evacuation and shelter-in-place orders, testing sustained response capabilities and population protection measures.
Evaluation Methodology
Performance assessment utilized a structured 3-tier rating system: “Achieved” for objectives fully met with correct and efficient actions and seamless communication; “Partially Achieved” for objectives partially met with notable gaps requiring improvement; and “Not Achieved” for objectives not met with incorrect or inefficient actions and significantly flawed communication. Trained observers from WHO evaluated responses against predefined criteria including timeliness, adherence to standard operating procedures (SOPs), and interagency communication effectiveness.
Results
Inject 1: Accident notification and initial response (achieved)
Initial notification protocols functioned effectively, with the special emergency commission activated and alerts issued to all relevant agencies within established timeframes. However, a critical gap was identified: the region lacking nuclear facilities had no established regular drills for radiological-nuclear emergencies, unlike regions with nuclear power plants that conduct routine preparedness exercises. Participants relied on general emergency procedures and existing legal frameworks, highlighting the need for specialized radiological emergency training across all regions regardless of nuclear facility presence.
Inject 2: Public communication and media management (achieved)
Coordination between agencies proved effective in managing public information and controlling misinformation through established channels, including press conferences, Telegram channels, and official social media platforms. However, significant challenges emerged regarding potassium iodide (KI) procurement and distribution. Participants identified unclear procurement responsibilities, inadequate storage planning, and distribution logistics gaps. Specific issues included centralized KI procurement in Kyiv without effective pharmacy network distribution and challenges with commercial pharmacy operations during emergencies.
Inject 3: Medical response and referral pathways (achieved)
Medical triage and referral pathways demonstrated functional capacity, with hospitals successfully activating mass casualty protocols and establishing communication for patient referrals. Critical weaknesses included staff hesitancy to respond due to fear of radiation exposure, inadequate social protection and insurance policies for medical personnel and first responders, and absence of standardized SOPs for handling contaminated materials and waste disposal. Hospitals lacked designated areas for contaminated material storage and contracts with specialized waste management companies for contaminated water disposal.
Inject 4: Communication with national health institutions (partially achieved)
Data exchange between first responders and national health institutions revealed delays due to information duplication and validation requirements during emergencies. The Ukrainian Scientific and Practical Center for Emergency Medical Care and Disaster Medicine demonstrated ongoing development of digital health information systems for emergency coordination, but gaps in real-time communication protocols were identified. International Medical Corps highlighted capacity-building efforts, having trained over 800 health care employees, but resource acquisition challenges persisted.
Inject 5: International assistance and resource mobilization (partially achieved)
Integration of international support showed mixed results. While international organizations demonstrated readiness to provide assistance, delays in deployment were identified due to lengthy procurement procedures and strict security measures under martial law conditions. Communication channels between international and national partners functioned adequately, but coordination mechanisms required refinement for rapid resource mobilization during radiological emergencies.
Inject 6: Prolonged evacuation and shelter-in-place orders (achieved)
Evacuation coordination proved effective for the simulated 10,000-person evacuation from a 30-kilometer radius, with successful phased evacuation planning and traffic management by the Ministry of Internal Affairs. However, hospitals faced significant challenges including delays in patient discharge due to extensive paperwork requirements and potential patient data loss during chaotic evacuations. Many facilities lacked cloud-based data backup systems, relying solely on on-site servers vulnerable to evacuation scenarios.
Quantitative Performance Assessment
Of 6 major exercise objectives, 4 were rated as “Achieved” and 2 as “Partially Achieved,” with no objectives rated as “Not Achieved.” Specific performance gaps included: 100% of participating regions lacked regular radiological emergency drills, 75% of hospitals reported inadequate staff insurance coverage for radiological response, and 60% of facilities lacked standardized decontamination SOPs. Communication response times averaged 15-20 minutes for initial notifications, meeting established benchmarks, while patient referral coordination required 30-45 minutes, exceeding optimal timeframes.
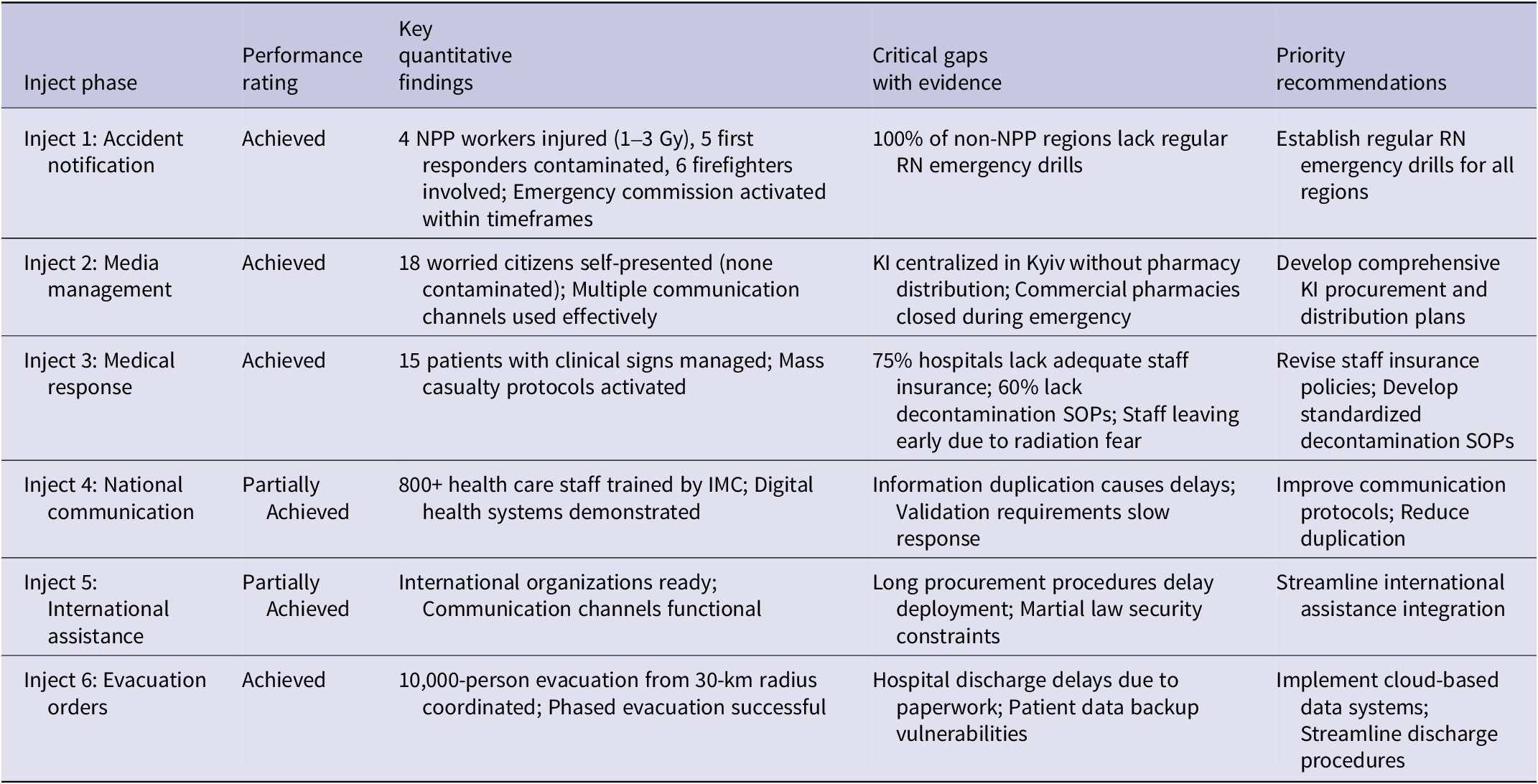
Table 1 provides a comprehensive performance assessment of all 6 exercise injects, consolidating key findings, identified gaps, and evidence-based recommendations derived from the September 2024 tabletop exercise. The structured evaluation framework employed standardized criteria (Achieved, Partially Achieved, Not Achieved) to assess each inject’s objectives, while quantitative evidence from participant observations and postexercise debriefings supports the identification of critical preparedness gaps. This systematic approach enables direct linkage between observed performance deficiencies and priority recommendations, providing actionable insights for emergency preparedness policy development and resource allocation decisions.
Table 1. Tabletop exercise performance assessment: Radiological emergency preparedness capabilities and identified gaps in Ukraine

• Exercise Performance Summary: Tabletop Exercise Assessment of Radiological Emergency Preparedness Capabilities in Ukraine with Specific Evidence from TTX Implementation. Performance ratings based on structured evaluation criteria with quantitative findings from the September 2024 exercise involving 12 organizations. IMC = International Medical Corps; KI = potassium iodide; NPP = nuclear power plant; RN = radiological-nuclear; SOPs = standard operating procedures.
• Performance assessment based on WHO observer evaluation using predefined criteria.
• Exposure levels: 1-3 Gray (Gy) for NPP workers, <1 Gy for first responders.
These findings, while demonstrating significant preparedness capabilities, also reveal several limitations that must be considered when interpreting the exercise results.
Limitations
Several factors limited the comprehensiveness of this assessment. The absence of key stakeholders, including the The Ukrainian Hydrometeorological Center (UHMC) (responsible for atmospheric monitoring and dispersion modeling), National Police (crowd control and security), Armed Forces of Ukraine (logistics and evacuation support), and Security Service of Ukraine (threat assessment and coordination), prevented full system testing and may have resulted in overestimation of current readiness levels. The fictional nuclear facility setting, while necessary for security reasons, could not replicate the full complexity of actual plant-specific emergency procedures and site-specific challenges. These limitations were addressed through scenario adaptations and role-playing by available participants to maintain exercise integrity while acknowledging gaps in comprehensive system testing.
The exercise duration of 3 days, while intensive, could not fully simulate the sustained response requirements of prolonged radiological emergencies that may extend for weeks or months. Additionally, the simulation could not replicate the psychological stress and fatigue factors that would affect real-world performance during actual radiological incidents. The evaluation methodology, while structured, relied on observer assessment rather than objective performance metrics, potentially introducing subjective bias in ratings.
Discussion
The TTX findings align with international literature emphasizing the critical importance of regular simulation exercises for maintaining radiological emergency preparedness.Reference Skryabina, Reedy, Amlôt, Jaye and Riley8
Comparative analysis with similar exercises conducted in other countries reveals common challenges in interagency coordination and public information management, particularly in regions without nuclear facilities.Reference Jackson and McKay9 The identified gaps in KI distribution planning reflect broader international challenges in pharmaceutical countermeasure deployment during radiological emergencies, as documented in post-Fukushima assessments.Reference Elvegård and Andreassen10
The staff hesitancy observed during medical response scenarios mirrors findings from radiological emergency exercises in other countries, where health care workers’ concerns about radiation exposure consistently emerge as a limiting factor in response effectiveness.Reference Skryabina, Reedy, Amlôt, Jaye and Riley8 The insurance and social protection gaps identified represent a unique challenge in Ukraine’s current operational environment, where traditional emergency response frameworks must adapt to wartime conditions while maintaining radiological preparedness capabilities.
The exercise demonstrated that Ukraine’s existing emergency response infrastructure provides a solid foundation for radiological emergency management, consistent with WHO assessments of national health emergency preparedness.2 However, the specific technical requirements of radiological emergencies require specialized training, equipment, and procedures that extend beyond general emergency response capabilities. This finding supports the WHO REMPAN framework’s emphasis on specialized radiological emergency preparedness as a distinct component of overall emergency management systems.Reference Carr5
The communication effectiveness observed during the exercise reflects the maturity of Ukraine’s emergency communication systems, developed through extensive experience with various emergency scenarios during the ongoing conflict. However, the technical complexity of radiological emergency communication, including dose assessment reporting and contamination status updates, requires specialized protocols that were not fully tested due to exercise limitations.
Conclusion
This TTX successfully demonstrated Ukraine’s foundational emergency response capabilities while identifying specific areas requiring enhancement for effective radiological emergency management. The exercise revealed that regions without nuclear facilities require dedicated radiological emergency preparedness programs to ensure comprehensive national response capacity.
Critical recommendations include: establishing regular radiological-nuclear emergency drills for all regions regardless of nuclear facility presence; developing comprehensive KI procurement, storage, and distribution plans with clear agency responsibilities; revising insurance and social protection policies for medical personnel and first responders engaged in radiological emergency response; creating standardized SOPs for contaminated material handling and waste disposal; implementing cloud-based patient data backup systems to prevent information loss during evacuations; and enhancing specialized training programs for health care workers in radiological emergency medical response.
The exercise validated the effectiveness of structured simulation exercises in identifying preparedness gaps and testing interagency coordination mechanisms. Regular implementation of similar exercises, with expanded stakeholder participation including military and meteorological services, will be essential for maintaining and improving Ukraine’s radiological emergency preparedness capabilities.
Future exercises should incorporate longer-duration scenarios to test sustained response capabilities, include actual hospital-based drills to complement tabletop simulations, and expand to test the scalability of response strategies from local to national levels. The integration of international assistance mechanisms requires particular attention to ensure rapid deployment capabilities while maintaining security protocols appropriate to Ukraine’s current operational environment.
Acknowledgments
The authors gratefully acknowledge the support of the Humanitarian Aid department of the European Commission (ECHO) and Canada’s Weapons Threat Reduction Program for their contributions to this initiative. Special recognition is extended to all participating organizations and their personnel who dedicated time and expertise to this critical preparedness assessment.
Author contribution
KA: Conceptualization, formal analysis, methodology, and writing; LNM: conceptualization, formal analysis, methodology, visualization, writing—original draft and review and editing; ZK, YL, AE, FAC, PB, and EB: writing—review and editing; and JH: supervision, writing—review and editing.
Competing interests
The authors declare none.

 Open access
Open access